J. Perinat. Med. 40 (2012) 311–314 • Copyright © by Walter de Gruyter • Berlin • Boston. DOI 10.1515/jpm-2011-1000
Intermittent fl ushing improves cannula patency compared to
continuous infusion for peripherally inserted venous catheters
in newborns: results from a prospective observational study
Anna Pereza, Isabelle Feuza, Barbara Brotschi
and Vera Bernet *
Department of Pediatric Intensive Care and Neonatology , Zurich University Children ’ s Hospital, Steinwiesstrasse, Zurich , Switzerland
Abstract
Aims: Peripheral cannulas in newborns are commonly used for intravenous treatment. However sustained maintenance of cannula patency is often diffi cult to achieve in this age group. This study compares the duration for which cannula patency can be maintained in newborns under continuous infusion, or an intermittent fl ushing regimen, with normal saline. Methods: A prospective observational study was conducted during a 12-month period. All newborns admitted to the 16-bed intermediate care unit, who required intravenous treatment, received either continuous peripheral infusion with 0.9 % saline at an infusion rate of 2 mL/h or an intravenous cannula, which was fl ushed with 1 mL of 0.9 % saline at least once every 24 h.
Results: A total of 53 patients with 86 cannulas were included. Twenty-fi ve (47 % ) patients received 41 continuous infusions. The intermittent fl ushing group consisted of 28 (53 % ) patients with 45 cannulas administered. The cannula patency was sig-nifi cantly longer in the intermittent fl ushing group (mean 62.1 vs. 92.8 h, P = 0.01). The patient ’ s underlying disease and the cannula insertion site were not related with the duration of the cannula patency.
Conclusions: Our study shows that intermittent cannula fl ushing is associated with improved cannula patency for peripherally inserted venous catheters in newborns.
Keywords: Cannula patency; continuous infusion; intermit-tent fl ushing; newborns; peripheral intravenous catheter.
Introduction
Peripheral cannulas are commonly used in newborns for the intravenous application of fl uids and drugs. Intravenous can-nulation and therapy with continuous infusion may require the newborn to be separated from its mother and can delay the establishment of maternal infant bonding [4, 9] . In new-borns requiring drug administration, but no continuous fl uid therapy, intermittent use of the cannula enables intravenous treatment in an ambulatory setting, which prevents separa-tion of mother and newborn and alleviates the necessity of the parent ’ s presence in the ward. Repeated venous access can be diffi cult to achieve in this patient group over time and is a stressful experience for the newborn, the new parents and the medical staff [5, 10] . Therefore, sustained maintenance of cannula patency is an imperative for prolonged intravenous treatment. Not much information on the different means of maintaining intravenous cannula patency is available in the literature. In a Cochrane review in 2005, Flint et al. focused on factors that infl uence the longevity of venous peripheral access and compared the outcome of continuous infusion to that of intermittent fl ushing. They were not able to establish that either method was superior to the other [1] .
The primary goal of the present study was to compare the duration of initial cannula patency under continuous infusion, in comparison to intermittent fl ushing with normal saline solution. In addition, the total number of cannulas inserted, the duration of total cannula patency, role of the underlying disease, weight and age of the newborn, as well as the cannula insertion site were investigated.
Patients and methods
The present prospective observational study analyzed the impact of two different treatment regimes on the patency of peripherally inserted venous cannulas in newborns. The study was conducted in the 16-bed neonatal intermediate care unit of a university teaching children ’ s hospital during a 12-month period using a convenience-based sampling strategy. The study was approved by the local Ethical Committee.
During the fi rst 6 months of the study (July–December 2008), all newborns admitted to the unit who required intravenous treatment, received continuous peripheral infusion with 0.9 % saline, at an infu-sion rate of 2 mL/h. During the course of the following 6 months (January–July 2009) all admitted newborns requiring peripheral injection of drugs were treated via an intravenous cannula, which was fl ushed with 1 mL of 0.9 % saline at least once every 24 h. If the newborn required antibiotics, the cannula was fl ushed with 1 mL saline after each drug application, respectively every 8 h. In all cases aShared fi rst authorship.
*Corresponding author: Vera Bernet, MD
Department of Pediatric Intensive Care and Neonatology Zurich University Children ’ s Hospital
Steinwiesstrasse 75 8032 Zurich Switzerland Tel.: + 41 44 266 7053 Fax: + 41 44 266 7168 E-mail: [email protected]
312 Perez et al., Cannula patency of peripherally inserted venous catheters in newborns
a 24-gauge, 19 mm long peripheral catheter (Insyte-N BD, Becton Dickinson, Allschwil, Switzerland) was used with a 10 cm long sy-ringe pump infusion line (Syramed line, Arcomed AG, Switzerland) and a three-way stopcock (Discofi x C-3, Braun AG, Switzerland). All cannulas were secured and controlled according to the hospital protocol, including fi xation on a splint if the cannula was inserted in the back of the hand, foot or crook of the elbow. For each treatment regimen the following measures were noted: gestational age, age at insertion of fi rst cannula, being born small for gestational age (SGA), weight of the newborn, underlying disease, date and time of cannula insertion, insertion site, date, time and reason of cannula removal. For the statistical analysis, the cannula insertion site was defi ned as “ distal ” , corresponding to the back of the hand or foot vs. “ proxi-mal ” , corresponding to the crook of the elbow or scalp. Concerning the newborn ’ s underlying disease we only investigated whether or not sepsis was present during the investigation period. Sepsis was defi ned as the presence of positive blood cultures, clinical signs with temperature instability, mottled or pale skin, irritability and signs of infection in the blood sample. We focused on the infl uence of sepsis on cannula patency and removal, suggesting that a patient with sep-sis and therefore bacteremia might be more susceptible to develop phlebitis and/or local infection at the site of foreign material in his blood stream.
Statistics
Statistical analysis was performed with SPSS, Version 16.0, using the Mann-Whitney non-parametric test for independent samples and multiple linear regressions for risk factor analysis with a statistical signifi cance defi ned by P < 0.05.
Results
During the fi rst 6-month study period, 25 patients receiving a total of 41 continuous infusions were included. During the second 6-month period, 28 patients with a total of 45 cannulas were included, the intravenous cannula being intermittently
fl ushed with 0.9 % saline. Gestational age was equally dis-tributed among the two treatment groups (P = 0.43) and there was no difference with regard to newborns being born small for gestational age (SGA) between the two treatment groups (intermittent fl ushing group: 1/28, continuous infu-sion group: 2/25; P = 0.60). Gestational age and SGA showed no statistically signifi cant effect on duration of cannula pat-ency when entered into the regression analysis (P = 0.32 and P = 0.47, respectively). There were no differences in body weight or time of initial cannula insertion between the two treatment groups (Table 1A). There were signifi cantly more sepsis patients in the intermittent fl ushing group (71.4 % ) than in the group treated with continuous infusion (40 % ; P = 0.03). The initial insertion of the intravenous cannula in both groups took place at the back of the hand (n = 31) or foot (n = 10), in the crook of the elbow (n = 7) or in the scalp (n = 5) and there was no statistically signifi cant difference between the two treatment groups with respect to insertion site of the initial cannula (P = 0.18). There was also no statistically signifi cant difference in the total number of employed cannulas between the treatment groups (P = 0.51). Inserted cannulas were removed for reasons of infi ltration/extravasation, occlusion, phlebitis or because they were no longer required. There was no difference in reasons for loss of function for the initially inserted cannulas between the treatment groups (P = 0.11). In the continuous infusion group the reasons for loss of cannula function were distributed as follows: 14 (56 % ) infi ltration, 3 (12 % ) phlebitis, 2 (8 % ) occlusion and 6 (24 % ) intact can-nula removal, because it was no longer required. The corre-sponding fi gures for the intermittent fl ushing group were: 12 (42.9 % ) infi ltration, 2 (7.1 % ) occlusion and 14 (50 % ) intact cannula removal, because it was no longer required.
The cannulas employed in the intermittent fl ushing group retained their patency for a signifi cantly longer period than did those employed in the continuous infusion group, with respect to both the initially inserted and the total number of
Table 1A Demographic data and main results for the initial cannula per patient.
Treatment group P-value
Continuous infusion (n = 25) Intermittent fl ushing (n = 28)
Patient weight in g (mean ± SD) 3375 ± 814 3435 ± 588 0.85
Patient age at fi rst cannula in days (mean ± SD) 12.1 ± 9.5 14.5 ± 8.2 0.28
Cannula insertion site 0.18
Distal site (n/ % ) 21/84 27/96.4
Proximal site (n/ % ) 4/16 1/3.6
Sepsis (n/ % ) 10/40.0 19/71.4 0.03
Cannula patency in hours (mean ± SD) 62.1 ± 44.3 92.8 ± 55.7 0.01
Table 1B Main results for the total of cannulas per patient.
Treatment group P-value
Continuous infusion (n = 41) Intermittent fl ushing (n = 45)
Sepsis (n/ % ) 19/46.3 33/75.0 0.016
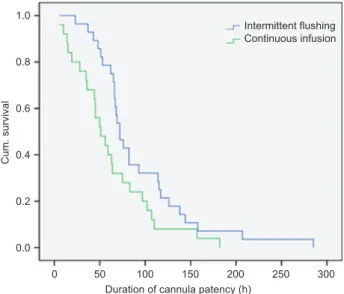
Perez et al., Cannula patency of peripherally inserted venous catheters in newborns 313 1.0 0.8 0.6 0.4 Cum. survival 0.2 0.0 0 50 100 200 300 Intermittent flushing Continuous infusion 150
Duration of cannula patency (h) 250
Figure 1 Kaplan-Meier survival curve for duration of cannula pat-ency in hours.
cannulas per individual patient (P = 0.01 and P = 0.002, respec-tively: Tables 1A and 1B ). The Kaplan-Meier curve depicts the statistically signifi cant difference in the duration of can-nula patency between the two treatment regimens (log rank test 0.032: Figure 1 ). Cannula insertion site, gestational age, being born SGA, age and weight of the newborn, had no effect on the longevity of cannula patency (P = 0.44, P = 0.32, P = 0.47, P = 0.51 and P = 0.46, respectively). Sepsis did not infl uence the duration of cannula patency (P = 0.37).
Discussion
The aim of the present study was to compare the duration of peripheral venous cannula patency in newborns under two different conditions (continuous infusion vs. intermittent fl ushing). We could demonstrate that patency was retained for a signifi cantly longer duration upon intermittent fl ushing than upon continuous infusion. This increased longevity applied to both the initially inserted cannula as well as to the total num-ber of applied cannulas per individual newborn.
A Cochrane review published by Flint et al. in 2005 included the only two controlled randomized trials compar-ing continuous infusion with intermittent fl ushcompar-ing, in order to prevent loss of function of peripheral intravenous cannu-las in newborns requiring drug administration [1] . One of the included studies describes similar duration of cannula pat-ency in both treatment groups for the fi rst cannula used per newborn. However, almost twice as many cannulas were used in the continuous infusion group compared to the intermittent fl ushing group [2] . In the second randomized trial, patency duration of the fi rst cannula used per infant was not reported. The duration of cannula patency was, in accordance with our fi ndings, signifi cantly longer in the intermittent fl ushing group (P-value = 0.0003), for all catheters averaged during the treatment course. The mean number of catheters used, defi ned
for the fi rst 48 h of treatment, was signifi cantly higher in the continuous infusion group [8] . In conclusion, the data of the Cochrane review were not able to establish that either method was superior to the other [1] , but the results support the use of intermittent fl ushing with saline 0.9 % in newborns requiring drug administration. This is in accordance with our fi ndings.
Similar results were also reported in a retrospective cohort study conducted in 2003. Flint et al. compared the duration of cannula patency for continuous infusion vs. intermittent fl ush-ing in term newborns requirush-ing intravenous medication only. Their study design was very similar to ours even though the fl ushing interval was shorter than in our study (6 h vs. 8 – 24 h, respectively). The study demonstrated that intravenous can-nulas last just as long if they are fl ushed intermittently with sodium chloride and do not have a continuous infusion run-ning. After the intermittent fl ushing regimen was established, the authors report the observation of various benefi ts includ-ing easy access for mothers to initiate early feedinclud-ing, greater involvement of parents in infant care, potential cost savings, and enhanced maternal-infant bonding.
In our study, the reasons for loss of function for the fi rst cannula used per newborn were similarly distributed between the two treatment groups. This is in contrast to the fi ndings of both studies included in the Cochrane review. Kalyn et al. report a statistically signifi cant difference (P-value < 0.001): in the intermittent fl ushing group catheters were less likely to infi ltrate, leak or develop phlebitis whereas in the continuous infusion group they were less likely to occlude [2] . Taylor et al. [8] focus on extravasation, defi ned as the number of infi l-trations per day. They report the mean of infi ll-trations a day to be signifi cantly higher in the continuous infusion group com-pared to the intermittent fl ushing group (P-value = 0.0015).
When we analyzed the newborns ’ underlying disease in our study, there were signifi cantly more sepsis patients in the intermittent fl ushing group compared to the continuous infu-sion group. However, no difference was shown in the reasons for loss of cannula function for the fi rst cannula used per new-born between the two treatment groups. Furthermore, sepsis did not infl uence the duration of cannula patency.
A number of trials have investigated the role of heparin in peripheral venous catheters of the newborn [3, 6, 7] . No heparin was used in either of our treatment groups, thus this was no object of investigation.
One limitation to our study is that we investigated two dif-ferent treatment methods in two separate time periods, which could possibly lead to a bias due to unrecognized temporal changes on our intermediate neonatal care unit. However, even if subtle changes over time cannot be completely excluded, there were certainly no major shifts in staff and/or treatment policies on the unit during the 12-month period of investigation.
The conclusion which can be drawn from the results of our study and with respect to previously published data [1, 2] in the literature is the following: intermittent cannula fl ushing may be associated with increased duration of cannula pat-ency for peripherally inserted venous catheters in newborns. This application modus has not shown any disadvantages and potentially allows intravenous treatment in an ambulatory
314 Perez et al., Cannula patency of peripherally inserted venous catheters in newborns
setting. The current data support the use of intermittent fl ush-ing of cannulas in selected populations of neonatal nurser-ies requiring drug administration only. However, in order to establish a new gold standard of care for peripheral venous cannulation in newborns, adequately powered randomized controlled trials will be needed.
References
[1] Flint A, McIntosh D, Davies MW. Continuous infusion versus intermittent fl ushing to prevent loss of function of peripheral intravenous catheters used for drug administration in newborn infants. Cochrane Database of Systematic Reviews. 2005. Art. No.: CD004593. DOI: 10.1002/14651858.CD004593.pub2. [2] Kalyn A, Blatz S, Pinelli J. A comparison of continuous
infu-sion and intermittent fl ushing methods in peripheral intravenous catheters in neonates. J Intraven Nurs. 2000;23:146 – 53. [3] Klenner AF, Fusch C, Rakow A, Kadow I, Beyersdorf E, Eichler
P, et al. Benefi t and risk of heparin for maintaining peripheral venous catheters in neonates: a placebo-controlled trial. J Pediatr. 2003;143:741 – 5.
[4] Levene MI, Tudehope DI, Thearle MJ. Parent-infant attachment and support for parents experiencing perinatal loss. In: Malcom IL, Tudehope DI, Thearle MJ, editors. Essentials of neonatal medicine. 3 rd ed., Oxford, Malden, MA: Blackwell Science; 2000. pp. 297 – 303.
[5] Olds SB, London ML, Ladewig PW. The newborn at risk: conditions present at birth. In: Olds SB, London ML, Wieland Ladewig PA, editors. Maternal-newborn nursing: a family and community-based approach. 6 th ed., Upper Saddle River, NJ: Prentice Hall Health; 2000. pp. 804 – 903.
[6] Randolph AG, Cook DJ, Gonzales CA, Andrew M. Benefi t of heparin in central venous and pulmonary artery cath-eters: a meta-analysis of randomized controlled trials. Chest. 1998;113:165 – 71.
[7] Shah PS, Ng E, Sinha AK. Heparin for prolonging periph-eral intravenous catheter use in neonates. Cochrane Database of Systematic Reviews. 2005. Art. No.: CD002774. DOI: 10.1002/14651858.CD002774.pub2.
[8] Taylor J, Shannon R, Kilbride HW. Heparin lock intravenous line. Use in newborn infants. A controlled trial. Clin Pediatr (Phila). 1989;28:237 – 40.
[9] WHO. Evidence for the ten steps to successful breastfeeding. Revised. 1998:278 – 92.
[10] Yeo H. Stress in the neonatal unit. In: Yeo H, editor. Nursing the neonate. Oxford, Malden, MA: Blackwell Science; 1998. pp. 278 – 92.
The authors stated that there are no confl icts of interest regarding the publication of this article.
Received May 3, 2011. Revised October 16, 2011. Accepted December 12, 2011. Previously published online January 19, 2012.