Invited Commentary
A. Buisson*,†,‡& L. Peyrin-Biroulet‡ *Department of Hepato-Gastroenterology, University Hospital Estaing of Clermont-Ferrand, Auvergne University, Clermont-Ferrand, France.
†Microbes, intestine, inflammation
and susceptibility of the host, UMR Inserm/Université d’Auvergne U1071, USC-INRA 2018, Clermont Université Clermont-Ferrand, France.
‡Inserm U954 and Department of
Hepato-Gastroenterology, University Hospital of Nancy, Université Henri Poincaré 1, Vandoeuvre-lès-Nancy, France. E-mail: [email protected] doi:10.1111/j.1365-2036.2011.04991.x
Complementary and alternative medicine in inflammatory bowel disease
SIRS, We read with great interest the article by Weizman et al. on the use of
com-plementary and alternative medicine (CAM) and its impact on medication
adher-ence in inflammatory bowel disease (IBD).1
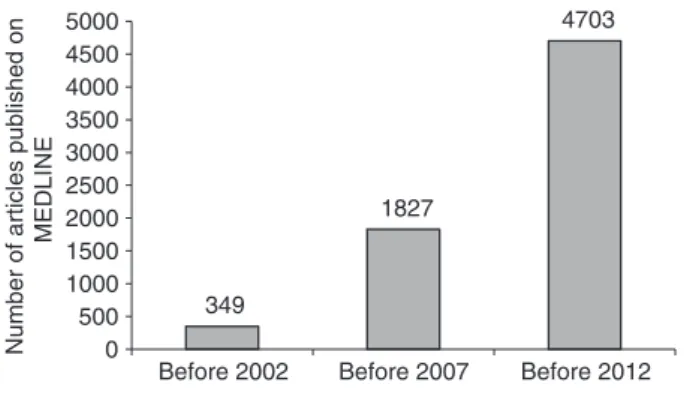
Over the past decade, the use of CAM has received increasing attention as reflected by the dramatic increase in the number of articles identified on
MED-LINE using the search terms “CAM” (Figure 1). A high rate (56%) of CAM use
was reported among IBD patients when compared to other chronic diseases such as cancers (40%), rheumatoid arthritis (38%), asthma (40%) and chronic renal
failure (25.2%).2–5 However, such discrepancy between these chronic conditions
may be partly explained by the fact that CAM defines a heterogeneous group of
medical practice. Accordingly, the European Crohn’s and Colitis Organisation (ECCO) recommended distinguishing complementary medicine (massage, relaxa-tion, meditation etc.…) from alternative medicine (Chinese medicine, herbal
products, probiotics etc.…).6
Even though CAM seems to have no impact on adherence to conventional therapy, limiting the use of costly and potentially life-threatening drugs should be a priority for all clinicians. Contrary to popular belief, natural therapies are not necessarily safe. Fatal hepatic and irreversible renal failure have occurred with
some preparations that may also interact with conventional medications.7
Fur-thermore, scientific evidence is usually missing regarding the efficacy of CAM,
even though herbal medicine appears promising in IBD.8
In this regard, the lack of information on safety and efficacy of CAM is a
major limitation to the study by Weizman et al.1 Rigorous randomised controlled
trials together with large prospective observational studies are needed to formally assess the benefit-risk ratio of CAM in IBD. Pending the results of these studies, the popularity of CAM among IBD patients challenges the physicians who should enhance their awareness and knowledge about this common practice to better advice their patients, especially the young women who were at increased risk of
using CAM referred to in the study by Weizman et al.1
AP&T invited commentary and correspondence columns are restricted to letters discussing papers that have been
pub-lished in the journal. A letter must have a maximum of 300 words, may contain one table or figure, and should have
no more than 10 references. It should be submitted electronically to the Editors via http://mc.manuscriptcentral.com/apt.
ª 2012 Blackwell Publishing Ltd 619
ACKNOWLEDGEMENTS
Declaration of personal interests: L. Peyrin-Biroulet has served as a speaker, a consultant and an advisory board member for Abbott and Merck. Declaration of funding interests: None.
REFERENCES
1. Weizman AV, Ahn E, Thanabalan R, Leung W, Croitoru K, Silverberg MS, et al. Characterisation of complementary and alternative medicine use and its impact on medication adherence in inflammatory bowel disease. Aliment Pharmacol Ther 2012;35: 342–9.
2. Horneber M, Bueschel G, Dennert G, Less D, Ritter E, Zwahlen M. How many cancer patients use complementary and alternative medicine: a systematic review and meta-analysis. Integr Cancer Ther 2011; doi: 10.1177/1534735411423920 [in press]. 3. Knoeller GE, Mazurek JM, Moorman JE.
Complementary and alternative medicine use among adults with work-related and non-work-related asthma. J Asthma 2011; doi:10.3109/02770903.2011.637597 [in press].
4. Ernst E, Posadzki P. Complementary and alternative medicine for rheumatoid arthritis and osteoarthritis: an overview of systematic reviews. Curr Pain Headache Rep 2011;15: 431–7.
5. Nowack R, Birck R. Complementary and alternative medicine is popular among chronic renal failure patients – renal
teams must increase their competence to advise patients with respect to efficacy and safety. Evid Based Nurs 2012; 15: 29–30.
6. Van Assche G, Dignass A, Reinisch W, van der Woude CJ, Sturm A, De Vos M, et al. The second European evidence-based consensus on the diagnosis and
management of Crohn’s disease: special situations. J Crohns Colitis 2010;4: 63– 101.
7. Langmead L, Rampton DS. Review article: complementary and alternative therapies for inflammatory bowel disease. Aliment Pharmacol Ther 2006;23: 341–9. 8. Fukunaga K, Hida N, Ohda Y, Takeda N,
Iimuro M, Yoshida K, et al. A prospective randomised double blind placebo controlled trial to assess the efficacy of a Chinese herbal medicine“Xilei San” as remission induction and maintenance therapy in patients with refractory ulcerative proctitis. Gastroenterology 2011; 140: S261. 349 1827 4703 0 500 1000 1500 2000 2500 3000 3500 4000 4500 5000
Before 2002 Before 2007 Before 2012
Number of articles published on
MEDLINE
Figure 1 | Number of articles related to complementary and alternative medicine published on MEDLINE before 2002, before 2007, and until the end of 2011.
620 Aliment Pharmacol Ther 2012; 35: 619-620 ª 2012 Blackwell Publishing Ltd