Norman
V. Carroll,
PhD*,Patrick Miederhoff,
PharmD, PhD*,Fred M. Cox,
PhDt,and
Jan D. Hirsch,
PhDt*School of Pharmacy, Virginia Commonwealth University, Medical College of Virginia, Richmond, Virginia; and tGlaxo Research Institute, Research Triangle Park, North Carolina
We examined patients‘ experiences with nausea and vomiting after they were discharged from outpatient surgical centers. Data were collected on 211 surgical outpatients at 24-48 h after discharge via a telephone interview conducted by outpatient surgery nurses, and at 5 days after discharge via a patient-completed ques- tionnaire. Telephone interviews were conducted with 193 patients. Questionnaires were completed by 154 pa- tients. Over 35% of patients experienced postdischarge nausea and vomiting. Most had not experienced nausea and vomiting in the recovery room. The severity of nau- sea for these patients averaged 5 on a lo-point scale (10 indicating very severe nausea). During the 5 days after
discharge, these patients reported experiencing nausea for an average of 1.7 days and vomiting for 0.7 days. Patients who experienced postdischarge nausea and vomiting were not able to resume their normal daily activities as quickly as those who did not. Patients man- aged postdischarge nausea and vomiting with little contact or intervention from health professionals and with minimal product purchases. The results indicate that postdischarge nausea and vomiting is common af- ter outpatient surgery, and that it results in substantial distress and impairment for patients who experience it.
(Anesth Analg 1995;80:903-9)
A
ccording to Rowbotham and Smith (l), post-operative nausea and vomiting are common and distressing postsurgical symptoms. These symptoms are of particular concern in outpatient sur- gery because they may require additional direct re- sources, such as supplies and antiemetic drugs, and because they may delay discharge. Of further concern, many patients experience postoperative nausea and vomiting after they have been discharged from the surgery center (l-4). This is especially troublesome because patients are much less accessible to profes- sional surveillance and care after discharge.
Although there is growing documentation of pa-
tients’ experiences with nausea and vomiting in the recovery room, there is little research on their experi- ences with postoperative nausea and vomiting after discharge. However, the few studies available suggest that nausea and vomiting is much more common post- discharge than in the recovery room (2-5). Due to the
This research was supported by the Glaxo Research Institute. Accepted for publication December 9, 1994.
Address correspondence and reprint requests to Norman V. Carroll, PhD, Professor of Pharmacy Administration, School of Pharmacy, Virginia Commonwealth University, MCV Box 533, Richmond, VA 23298.
medically unsupervised environment in which pa- tients complete their postsurgical recovery, and the potential complications that can stem from vomiting
(e.g., hematoma, wound dehiscence, pain), postdis- charge nausea and vomiting deserves closer scrutiny.
The purpose of this study was to examine patients’ experiences with nausea and vomiting after discharge from outpatient surgery centers. Specific objectives of the study were to determine:
1. The incidence of postdischarge nausea and vom- iting;
2. The extent to which postdischarge nausea and vomiting affect patients’ normal functioning and daily activities after ambulatory surgery; and 3. The ways in which patients manage and/or cope
with postdischarge nausea and vomiting.
Methods
Nurses employed in the outpatient surgical centers (OSCs) of six hospitals in the metropolitan area of a Southeastern city enrolled 211 patients into the study. Patients admitted to the OSCs from September 2,1992, through February 15,1993, were enrolled in the study if they met the following criteria: 1) 18 yr of age or
01995 by the International Anesthesia Research Society
Table 1. Demographic Description of the Patients Studied Postdischarge
nausea and Telephone interview sample
vomiting Yes (n = 57) No (n = 136)
Age (yr) 39.8 (13.3)* 44.4 (15.0)*
Weight (lb) 171.6 (42.7) 166.2 (33.8)
Female (%) 69.1 65.3
Values are mean (SD).
*Groups are significantly different at P = 0.05.
Questionnaire sample
Yes (n = 48) No (n = 106)
41.6 (14.6) 45.3 (14.4)
156.1 (32.6)* 170.4 (36.2)*
74.4 67.0
Table 2. Frequency of Surgical Procedures by Surgical Center
Center no.
1 2 3 4 5 6 Total
Procedure No. % No. % No. % No. % No. % No. % No. %
Laparoscopy 1 2.7 11 21.2 16 37.2 7 38.9 5 15.6 14 48.3 54 25.6 Dilation and 7 18.9 18 34.6 6 14.0 4 22.2 9 28.1 10 34.5 54 25.6 curettage Arthroscopy 26 70.3 18 34.6 11 25.6 7 38.9 6 18.8 4 13.8 72 34.1 Hernia repair 3 8.1 5 9.6 10 23.3 0 0.0 12 37.5 1 3.5 31 14.7 Total patients 37 52 43 18 32 29 211
Table 3. Most Frequently Used Drugs for Induction of Anesthesia
Center no.
1 2 3 4 5 6 Total
Anesthetic No. % No. % No. % No. % No. % No. % No. %
Propofol 23 62.2 48 92.3 24 55.8 18 100.0 20 62.5 27 93.1 160 75.8
Midazolam 26 70.3 32 61.5 38 88.4 12 66.7 27 84.4 11 37.9 146 69.2
Thiopental 0 0.0 0 0.0 1 2.3 0 0.0 11 34.4 2 6.9 14 6.6
Etomidate 0 0.0 0 0.0 1 2.3 0 0.0 0 0.0 0 0.0 1 0.5
Total patients 37 52 43 18 32 29 211
older; 2) surgery was performed under general anes- thesia; and 3) admitted for one of four selected sur- geries: laparoscopy, dilation and curettage, arthros- copy, or hernia repair. The latter two requirements were included because 1) higher rates of postoperative nausea and vomiting have been reported in patients undergoing general anesthesia (6-81, 2) the proce-
dures are frequently performed under general anes-
thesia in OSCs, and 3) they have been associated with appreciable rates of postoperative nausea and vomit- ing in the outpatient setting (2,4,7,9).
All participants signed informed consent forms. These forms, and the design of the study, were ap- proved by the Medical College of Virginia Committee on the Conduct of Human Research and by the
institutional review boards of the participating
hospitals.
Nurses recorded the number of episodes of vom- iting and estimated the severity of nausea for all
patients who experienced nausea or vomiting in the recovery room. Postdischarge data were collected for two different time periods. Nurses were instructed to call and interview patients by telephone on the day after discharge. The questionnaire used to conduct
the interview is shown as Appendix 1. Additional
data were collected by means of self-administered questionnaires which were given to patients at the time of discharge. Patients were instructed to com- plete and return the questionnaire 5 days after dis- charge. The patient self-administered questionnaire is
shown as Appendix 2.
Data analyses consisted of calculation of means,
SDS, and frequencies. 2 tests, Wilcoxon’s signed rank
tests, and one-way analysis of variance were used to test for significant differences between groups. Sta- tistical significance is reported at P < 0.05. Data analyses were performed with PC-SAS software (SAS Institute, Cary, NC).
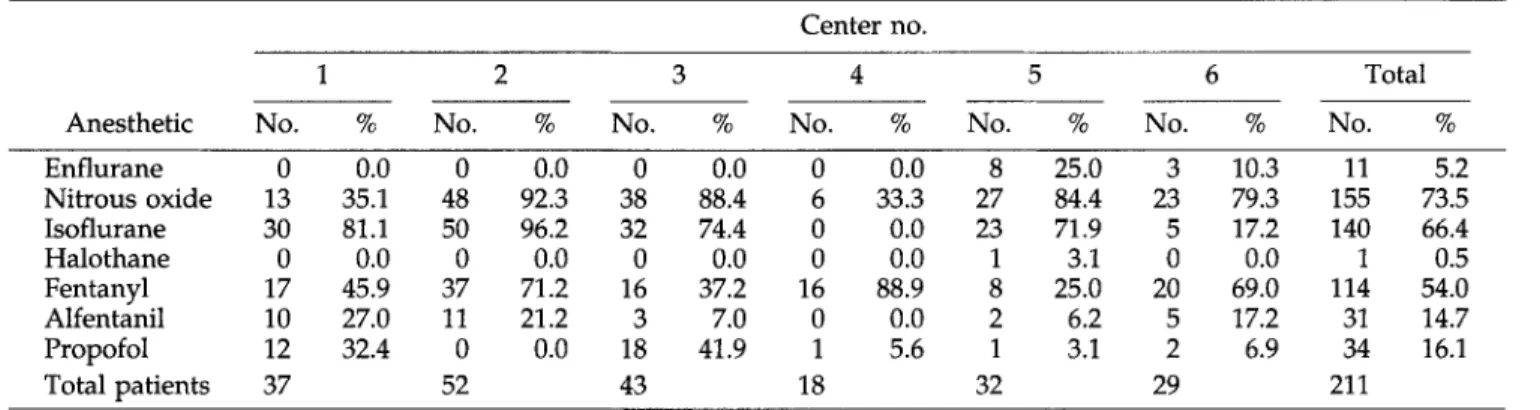
Table 4. Most Frequently Used Drugs to Maintain Anesthesia
Center no.
1 2 3 4 5 6 Total
Anesthetic No. % No. % No. % No. % No. % No. % No. %
Enflurane 0 0.0 0 0.0 0 0.0 0 0.0 8 25.0 3 10.3 11 5.2 Nitrous oxide 13 35.1 48 92.3 38 88.4 6 33.3 27 84.4 23 79.3 155 73.5 Isoflurane 30 81.1 50 96.2 32 74.4 0 0.0 23 71.9 5 17.2 140 66.4 Halothane 0 0.0 0 0.0 0 0.0 0 0.0 1 3.1 0 0.0 1 0.5 Fentanyl 17 45.9 37 71.2 16 37.2 16 88.9 8 25.0 20 69.0 114 54.0 Alfentanil 10 27.0 11 21.2 3 7.0 0 0.0 2 6.2 5 17.2 31 14.7 Propofol 12 32.4 0 0.0 18 41.9 1 5.6 1 3.1 2 6.9 34 16.1 Total patients 37 52 43 18 32 29 211
Table 5. Most Frequently Used Neuromuscular Blocking Drugs
Atracurium 4 10.8 1 1.9 9 20.9 2 11.1 23 71.9 16 55.2 55 26.1 Vecuronium 1 2.7 3 5.8 8 18.6 12 66.7 0 0.0 4 13.8 28 13.3 Succinylcholine 19 51.4 7 13.5 2 4.7 2 11.1 1 3.1 14 48.3 45 21.3 d-Tubocurarine 3 8.1 5 9.6 0 0.0 0 0.0 0 0.0 11 37.9 19 9.0 Gallamine 6 16.2 8 15.4 0 0.0 0 0.0 0 0.0 3 10.3 17 8.1 Mivacurium 2 5.4 0 0.0 12 27.9 0 0.0 0 0.0 2 6.9 16 7.6 None 16 43.2 35 67.3 13 30.2 5 27.8 9 28.1 2 6.9 80 37.9 Total patients 37 52 43 18 32 29 211 Center no. 1 2 3 4
No. % No. % No. % No. %
5 No. % 6 No. % Total No. %
Table 6. Times at Which Nausea and/or Vomiting Were Experienced by 143 Patients Completing Both Telephone Interview and Questionnaire
Nausea and vomiting
Postdischarge Time No. %
No None 85 59.4
Recovery room only 7 4.9
Total 92 64.3
Yes Recovery room + postdischarge 14 9.8
Only <48 h postdischarge 24 16.8
Only >48 h-5 d postdischarge 13 9.1
Total 51 35.7
Total patients 143 100.0
Results
Telephone interviews were completed with 193 pa- tients (91.5% of patients enrolled in the study). The mean time elapsed between discharge and completion
of the telephone interview was 1.9 5 1.5 SD days.
Questionnaires were returned by 154 patients (73.0% of patients enrolled). The mean time elapsed between discharge and completion of the questionnaire was 5.1 + 2.8 days.
Table 1 compares demographic information for the groups who did and did not experience postdischarge nausea and vomiting and for the samples completing the telephone interview and questionnaire.
The frequencies with which the four surgical proce- dures were performed in each OSC are reported in
Table 2. The most frequently used anesthetics and
neuromuscular blocking drugs are reported in Tables 3-5.
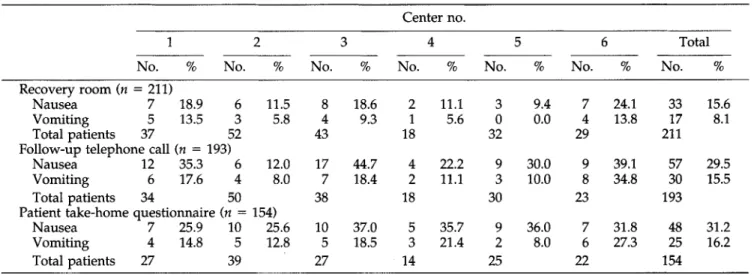
Fifty-seven (29.5%) of the 193 patients contacted by telephone and 48 (31.2%) of the 154 patients who returned questionnaires experienced nausea and vom- iting after discharge from the OSC. A total of 143 patients completed both the telephone interview and the 5-day follow-up questionnaire. Fifty-one of these patients (35.7%) experienced postoperative nausea and vomiting after discharge from the OSC (Table 6). The data in Table 7 show the incidence of nausea and vomiting for each surgical center and time period (recovery room, 24- to 48-h telephone call, and 5-day
questionnaire). Table 8 reports the severity and
duration of nausea and vomiting during each time period. Table 9 reports the rates of postdischarge
nausea and vomiting for each of the four surgical
Table 7. Incidence of Postoperative Nausea and Vomiting by Surgical Center and Time Period
Center no.
1 2 3 4 5 6 Total
No. % No. % No. % No. % No. % No. % No. %
Recovery room (n = 211)
Nausea 7 18.9 6 11.5
Vomiting 5 13.5 3 5.8
Total patients 37 52
Follow-up telephone call (n = 193)
Nausea 12 35.3 6 12.0
Vomiting 6 17.6 4 8.0
Total patients 34 50
Patient take-home questionnaire (n = 154)
Nausea 7 25.9 10 25.6 Vomiting 4 14.8 5 12.8 Total patients 27 39 8 18.6 2 11.1 3 9.4 7 24.1 33 15.6 4 9.3 1 5.6 0 0.0 4 13.8 17 8.1 43 18 32 29 211 17 44.7 4 22.2 9 30.0 9 39.1 57 29.5 7 18.4 2 11.1 3 10.0 8 34.8 30 15.5 38 18 30 23 193 10 37.0 5 35.7 9 36.0 7 31.8 48 31.2 5 18.5 3 21.4 2 8.0 6 27.3 25 16.2 27 14 25 22 154
Table 8. Mean Severity and Duration of Nausea and Vomiting by Time Period
Telephone 5-Day follow-up
Recovery room interview questionnaire
Mean SD Mean SD Mean SD
Severity of nausea” Duration of nausea (days) No. of days on which vomiting
was experienced Episodes of vomiting 4.5 NA NA 0.8 2.3 1.2 5.5 2.8 4.7 2.6 1.3 0.8 1.7 1.3 0.7 1.1 0.7 0.8
Not measured Not measured
NA = not applicable.
’ Severity was measured on a IO-point scale for which 1 indicated no nausea and 10 indicated very severe nausea.
Table 9. Number and Percent of Patients Experiencing Postoperative Nausea and/or Vomiting by Time and Surgical Procedure
Surgical procedure
5-Day follow-up
Recovery room Telephone interview questionnaire
n No. % n No. % n No. %
Laparoscopy 54 16 29.6 47 20 42.6 36 20 55.6*
Dilation and curettage 54 5 9.4 50 8 16.0 46 8 17.4
Arthroscopy 72 12 16.7 65 20 30.8* 52 14 26.9
Hernia repair 31 1 3.6 31 9 29.0* 20 6 30.0*
Total 211 34 16.1 193 57 29.5 154 48 31.2
n = number in sample.
* P value from the signed rank test for related samples < 0.05.
Patients who experienced postdischarge nausea and/or vomiting reported minimal interventions to help them manage or cope with the problem. They seldom contacted health professionals. Of the 154 pa- tients who returned the 5-day questionnaire, only two reported calling a physician, one called the surgery center, and one visited a pharmacy. Purchases typi- cally cost little (Table 10) and no patient hired help.
Table 10. Number and Percent of Patients Making Purchases and Cost of Purchases for Treatment of Postdischarge Nausea and Vomiting
Type of purchase No. % Mean SD
Prescription medicines 2 4.2 $1.10 6.03
Over-the-counter medicines 4 8.3 $0.58 2.81
Beverages 11 22.9 $0.59 1.61
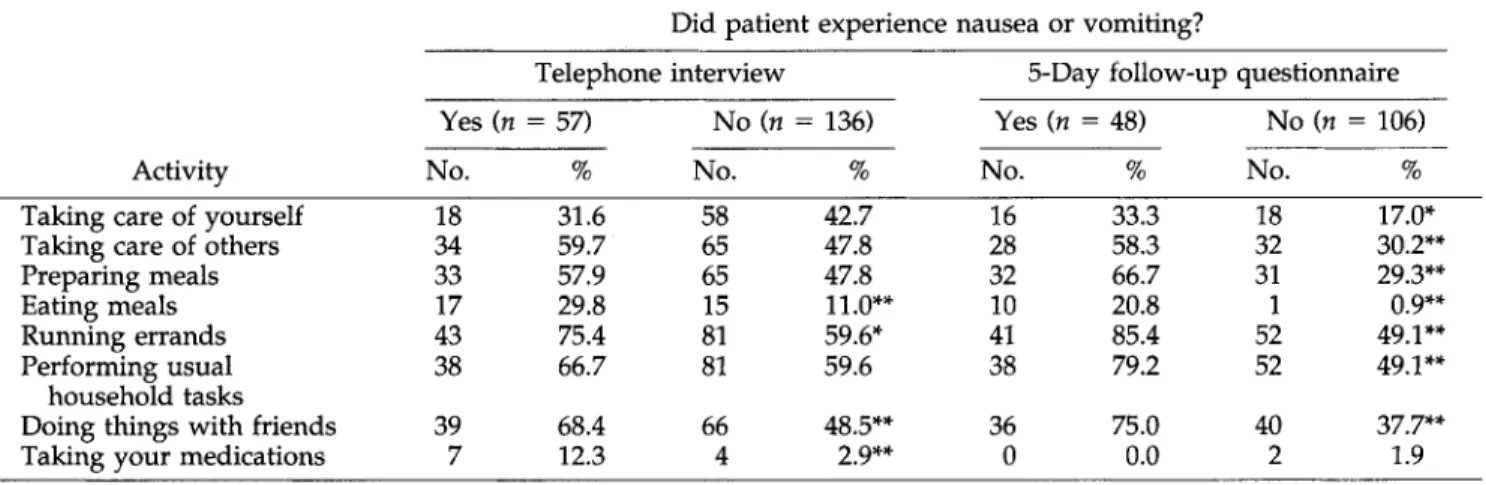
Table 11. Number and Percent of Patients Reporting Problems Performing Normal Daily Activities Did patient experience nausea or vomiting?
Telephone interview 5-Day follow-up questionnaire
Yes (n = 57) No (n = 136) Yes (n = 48) No (n = 106)
Activity No. % No. % No. % No. %
Taking care of yourself Taking care of others Preparing meals Eating meals Running errands Performing usual
household tasks Doing things with friends Taking your medications
18 31.6 58 42.7 34 59.7 65 47.8 33 57.9 65 47.8 17 29.8 15 11.0** 43 75.4 81 59.6* 38 66.7 81 59.6 39 68.4 66 48.5** 7 12.3 4 2.9** 16 33.3 18 17.0% 28 58.3 32 30.2** 32 66.7 31 29.3** 10 20.8 1 0.9** 41 85.4 52 49.1** 38 79.2 52 49.1** 36 75.0 40 37.7** 0 0.0 2 1.9 * P -c 0.05. ++P < 0.01.
Patients who reported experiencing nausea and vomiting in the 24- to 48-h period immediately after discharge were significantly more likely to have prob- lems performing their normal daily activities than were those not experiencing postdischarge nausea
and vomiting (Table 11). Differences between the
groups were more pronounced for the longer
postdischarge period reported on the questionnaire (Table 11).
Discussion
Postdischarge nausea and vomiting were experienced by more than 35% of patients in this study, many of whom had not experienced nausea and vomiting in the recovery room. During the 5-day period after dis- charge, these patients were significantly more likely to report impairment in performing their normal daily activities than were patients who did not experience nausea and vomiting. Despite the prevalence and per- ceived impact of postdischarge nausea and vomiting, few patients called health professionals for advice or purchased products to treat the problem. However,
lack of intervention does not necessarily indicate a
minimal problem. Patients in the study were coun- seled prior to discharge that nausea and vomiting might occur. They were, however, given only general instructions for management (e.g., dietary cautions, drinking carbonated beverages, taking pain medica- tions on a full stomach). Given that surgical outpa- tients are not under direct medical supervision during their postdischarge recovery period, and that signifi- cant nausea and vomiting, aside from being distress- ing, may place patients at risk for complications and impede resumption of normal activities, it may be prudent to provide patients with more detailed in-
structions for preventing or managing nausea and
vomiting episodes.
The present study was confined to patients under- going one of four procedures under general anesthesia in six surgical centers within one metropolitan area. The incidence, severity, duration, impact, and effec- tiveness of management techniques for postdischarge nausea and vomiting using larger and more diverse patient populations is unknown. The majority of pa- tients reporting problems in our study did not expe- rience nausea or vomiting until several hours after
discharge (with considerable variability in onset
among patients during the 5-day period). Further, there was little correlation between the occurrences of pre- and postdischarge nausea and vomiting. This may suggest a multifactoral etiology for postdischarge nausea and vomiting which may include not only the factors commonly associated with postoperative nau- sea and vomiting but additional factors, such as mo- tion, premature ambulation, and pain medications, which may come into play at various points during the postdischarge recovery period. Closer scrutiny of these factors may provide insight for identifying pa- tients most at risk for postdischarge nausea and vom- iting and for developing effective prophylaxis and intervention strategies.
Appendix
1
Questions Asked at 24-h Follow-up
Telephone Interview
1. Have you experienced any nuuseu or vomiting since leaving the center? Yes/No
2. How would you rate the severity of your nausea on a scale of 0 to 10 (with 0 being no nausea and 10 being very severe nausea)? (Circle only one number on the scale.)
No nausea Very severe nausea 0 1 2 3 4 5 6 7 8 9 10 I I I I I I I I I 3. 4. 5. 6. 7. 8. 9.
On how many different days have you been nau-
seated since you were discharged from the outpa-
tient surgical center? (If none, write in zero.)
On how many different days have you vomited
since you were discharged from the outpatient sur- gical center? (If none, write in zero.)
I am going to read a list of activities you might have
been prevented from doing as a result of your
surgery. Please tell me which of these you have not been able to do in the past 24 h because of your surgery.
A. Taking care of yourself B. Taking care of anyone else
C. Preparing meals
D. Eating meals
E. Running errands
F. Performing usual household tasks
G. Doing things with friends H. Taking your medications
Have you taken any prescription medicines for the
treatment of your nausea and vomiting since you
were discharged from the outpatient surgical cen-
ter? Yes/No
Please tell me all the prescription medicines you
have taken for the treatment of your nausea and
vomiting and when you last took each.
Have you taken any prescription medicines for the
treatment of your pain since you were discharged
from the outpatient surgical center? Yes/No
Please tell me all the prescription medicines you
have taken for the treatment of your pain.
Appendix
2
Questions from Patient
Self-Administered
Questionnaire
1. Have you experienced any nausea or vomiting
since leaving the surgery center? Yes/No
2. How would you rate the severity of your nausea on a scale of 0 to 10 (with 0 being no nausea and 10
being severe nausea)? (Circle only one number on
the scale.)
No nausea Very severe nausea
0 1 2 3 4 5 6 7 8 9 10
I I I I I I I I I
On how many different days, if any, have you
experienced nausea since being discharged from the
outpatient surgery center?
On how many different days, if any, have you
experienced vomiting since you were discharged
from the outpatient surgical center? (If none, write a zero in the blank below.)
Please circle the number beside all of the following
things which you have had to do since being dis-
charged as a result of nausea and/or vomiting. Also,
write in the number of different times you had to
do each thing:
1. Call a physicians office? No. of times 2. Call the surgery clinic? No. of times 3. Call a pharmacist? No. of times 4. Visit a physicians office? No. of times 5. Visit a pharmacy? No. of times
6. Visit an emergency room? No. of times
Please circle the number beside all of the following
items or services which you have had to buy to
treat the nausea and/or vomiting from your surgery.
Also indicate the amount you had to spend for
each. 1. 2. 3. 4. 5. 6.
Prescription medicines: Amount spent $
Over the counter medicines: Amount spent
$
Hired help: Amount spent $
Special beverages: Amount spent $
Special food(s): Amount spent $
Other purchases (please explain the type of other
purchases in the space below): Amount spent
$
7. On how many of the last 5 days were you unable to
carry out your normal responsibilities-such as
working, homemaking, or going to school-be-
cause of your surgery?
8.-12. Questions about employment of patient and
caregiver.
13. Which of the following activities were you pre-
vented from doing during the past 5 days as a
result of your surgery? (Circle all that you were
prevented from doing.)
1. Taking care of yourself 2. Taking care of anyone else
3. Preparing meals
4. Eating meals 5. Running errands
6. Performing usual household tasks
7. Doing things with friends 8. Taking your medications
14.-15. Questions about satisfaction with outpatient
16.-17. Questions about source of payment for medi- cal care and prescriptions.
References
1. Rowbotham DJ, Smith G. Introduction to supplement on post- operative nausea and vomiting. Br J Anaesth 1992;69(1 Suppl): 1s.
2. Lerman J. Surgical and patient factors involved in postoperative nausea and vomiting. Br J Anaesth 1992;69(1 Suppl):24S-32s. 3. Philip BK. Patients’ assessment of ambulatory anesthesia and
surgery. J Clin Anesth 1992;4:355-8.
4. Sanchez LA, Hirsch JD, Carroll NV, Miederhoff PA. Estimation of the cost of post-operative nausea and vomiting in an ambu- latory surgery center. J Res Pharmaceutical Economics 1994. In press.
5. Young ML, Kitz DS, Andrews R, et al. Efficacy of antiemetic prophylaxis in patients receiving general anesthesia for outpa- tient surgery. Anesthesiology 1988;69:3A.
6. Rabey PG, Smith G. Anaesthetic factors contributing to postop- erative nausea and vomiting. Br J Anaesth 1992;69(1 Suppl): 4oS-45s.
7. Wetchler BV. Postoperative nausea and vomiting in day-case surgery. Br J Anaesth 1992;69(1 Suppl):33S-39s.
8. Weinstein CM. Outpatient techniques. In: Klein SL, Landers DF, eds. Anesthesiology. East Oradell, NJ: Medical Economics Books, 1990~273-82.
9. Watcha MF, White PF. Postoperative nausea and vomiting. Anesthesiology 1992;77:162-84.