Review Article
Cervical Spine Involvement in Mild Traumatic Brain Injury:
A Review
Michael Morin,
1,2Pierre Langevin,
3,4and Philippe Fait
1,2,3,51Department of Human Kinetics, Universit´e du Qu´ebec `a Trois-Rivi`eres (UQTR), Trois-Rivi`eres, QC, Canada G9A 5H7 2Research Group on Neuromusculoskeletal Dysfunctions (GRAN), UQTR, Trois-Rivi`eres, QC, Canada G9A 5H7 3Cortex M´edecine et R´eadaptation Concussion Clinic, Quebec City, QC, Canada G1W 0C5
4Department of Rehabilitation, Faculty of Medicine, Laval University, Quebec City, QC, Canada G1V 0A6 5Research Center in Neuropsychology and Cognition (CERNEC), Montreal, QC, Canada H3C 3J7
Correspondence should be addressed to Philippe Fait; [email protected] Received 1 March 2016; Revised 30 May 2016; Accepted 19 June 2016 Academic Editor: S. John Sullivan
Copyright © 2016 Michael Morin et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background. There is a lack of scientific evidence in the literature on the involvement of the cervical spine in mTBI; however,
its involvement is clinically accepted. Objective. This paper reviews evidence for the involvement of the cervical spine in mTBI symptoms, the mechanisms of injury, and the efficacy of therapy for cervical spine with concussion-related symptoms. Methods. A keyword search was conducted on PubMed, ICL, SportDiscus, PEDro, CINAHL, and Cochrane Library databases for articles published since 1990. The reference lists of articles meeting the criteria (original data articles, literature reviews, and clinical guidelines) were also searched in the same databases. Results. 4,854 records were screened and 43 articles were retained. Those articles were used to describe different subjects such as mTBI’s signs and symptoms, mechanisms of injury, and treatments of the cervical spine. Conclusions. The hypothesis of cervical spine involvement in post-mTBI symptoms and in PCS (postconcussion syndrome) is supported by increasing evidence and is widely accepted clinically. For the management and treatment of mTBIs, few articles were available in the literature, and relevant studies showed interesting results about manual therapy and exercises as efficient tools for health care practitioners.
1. Introduction
Mild traumatic brain injury (mTBI) is commonly known as concussion [1]. In a recent study, Statistics Canada estimated mTBI annual incidence to be 600 per 100,000 people [1]. The pediatric TBI population is the patients’ subgroup who consulted the most often in the emergency room [1]. An estimated 1.6 to 3.8 million sport and recreation-related brain injuries occur in the United States annually, and up to 75% of them are classified as mild [2]. About 70 to 90 percent of all TBI cases are thought to be of mild severity, and the related symptoms usually resolve within 7 to 10 days [3, 4]. However, as many as 50% of concussions may go unreported [5]. In an epidemiologic study, Tator et al. (2007) reported that the highest incidence for TBI is in the age group under 18 years, with almost 45%. Additionally, approximately one-quarter of all patients with TBI are aged between 19 and 29 years [1].
The Centers for Disease Control and Prevention (CDC) describes mTBI as a silent epidemic [2].
Concussion in sports was defined in 2012 at the interna-tional consensus on concussion in sport held in Zurich as
a brain injury and is defined as a complex patho-physiological process affecting the brain, induced by biomechanical forces. Several common features that incorporate clinical, pathologic and biome-chanical injury constructs may be utilized in defining the nature of a concussive head injury. This is caused by a direct blow to the head, face, neck or elsewhere on the body with an “impulsive” force transmitted to the head. [4]
The number of reported concussions has increased in recent years for multiple reasons. Recent studies identified an increased awareness of the potential complications following
Volume 2016, Article ID 1590161, 20 pages http://dx.doi.org/10.1155/2016/1590161
concussion and repeated head trauma in the population [6] and higher involvement of health professionals in sports and in concussions recognition and follow-up [7]. Even though it is believed that most concussions usually resolve in between 7 and 10 days [3, 4], the symptoms may persist longer for up to 33 percent of cases [8]. Symptoms persisting for a few weeks to more than six months are defined in the literature as postconcussion syndrome (PCS) [8].
PCS is a complex medical subject that few articles and studies in the scientific literature explore concretely [4]. Con-sidering that mTBI is a multifaceted injury, many signs and symptoms complicate its diagnosis [3]. Multiple impairments linked to this condition such as cognitive, vestibular, cervical, physical, and psychological dysfunctions [3, 4]. Therefore, with a multitude of clinical theories in the literature, it is diffi-cult to determine clinical guidelines for PCS [3]. Current con-sensus identifies that a multidisciplinary approach is essential to the progress of the patient suffering from PCS [4].
One of the major challenges in the medical management of concussion is that there is no “gold standard” for assessing and diagnosing the injury [9]. It has been shown by Schneider et al. (2014) that a combination of cervical and vestibular physiotherapy decreased time to medical clearance for the return to sport in a cohort of 31 patients (12–30 years old) with persistent symptoms of dizziness, neck pain, and/or head-aches following a sport-related concussion [10]. However, little research has been published on this very specific topic.
2. Problem
The problem targeted by this review of literature is the lack of data regarding the association between mTBI and cer-vicogenic impairment. The majority of scientific publications focus on diagnosing mTBI, and there is little evidence on the possible involvement of the cervical region [4]. Cervical spine examination after a cranial trauma is essential, but the asso-ciation between symptoms and mTBIs is poorly described in the literature. A literature review will improve the medical knowledge of all medical professionals and help the diagnosis and treatment of mTBI.
3. Goals
The aim of this review was to target scientific articles describ-ing mTBI and those involvdescrib-ing cervicogenic headache (CGH) cases in order to look at the connections and similarities between these two types of injuries. The specific goals of this paper are (1) to determine the common signs and symptoms of mTBI (including PCS) and cervical dysfunctions, (2) to describe the mechanism of cranial trauma injury and link it with the impact on the cervical spine, and (3) to give an update on the various types of effective treatments for these conditions.
4. Methods
The following electronic resources were searched from Jan-uary 1, 1990, to May 19, 2015: PubMed, Index to Chiro-practic Literature (ICL), SportDiscus, Physiotherapy Evidence
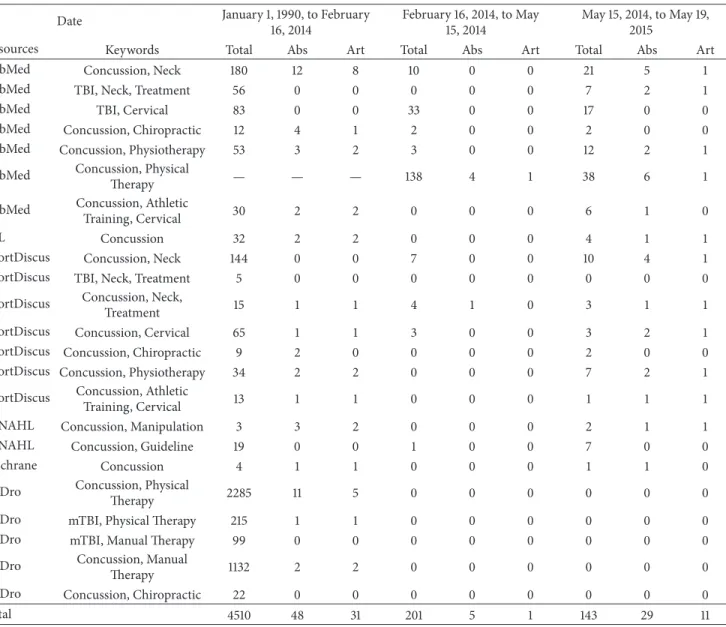
Database (PEDro), Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Cochrane Library databases. The following keywords were used in different combinations: concussion, neck, TBI, mTBI, cervical, physiotherapy, physical therapy, athletic training, treatment, chiropractic, manipula-tion, manual therapy, and guideline. For the complete list of combinations, see Table 1. Three data collections were carried out at different dates: February 16, 2014, May 15, 2014, and May 19, 2015. Reference lists of articles meeting the selection criteria were also collected. All abstracts in English and French dealing with concussion involving the neck were selected for a full reading of the article. A total of 4,854 abstracts were found on search engines. Following this search, the articles were selected according to three main streams:
(1) mTBI’s and PCS symptoms related to the cervical spine.
(2) Mechanism of injury.
(3) Therapies of the cervical spine with symptoms related to mTBI.
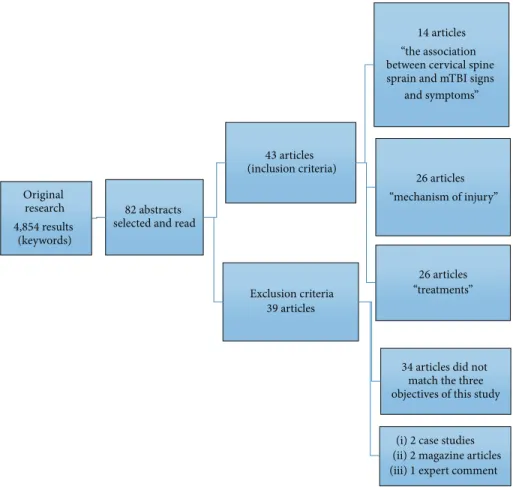
Inclusion criteria, based on the precited keywords, were original data articles, literature reviews, and clinical recom-mendations, available in English and/or French, based on the objectives of this research. Exclusion criteria were foreign language papers other than English or French, case studies, magazine articles, and expert and editorial comments. The selection of articles is shown in Figure 1, and combinations are explained in Table 1.
5. Results
After a careful screening of 4,854 data entries, 82 abstracts met the inclusion criteria of our research and were reviewed. All these articles were read and analyzed. Thirty-eight articles were excluded because the main topic did not match the three topics of this study (𝑛 = 34) or were case studies (𝑛 = 2), magazine articles (𝑛 = 2), and expert commentary (𝑛 = 1). Finally, 43 papers were included in this literature review. Each selected article is described in Table 2 (see Appendix). These articles were analyzed and assigned to the different categories of topics discussed: (1) the association between cervical spine sprain and mTBI signs and symptoms, (2) mechanism of injury, and (3) treatments. Results are represented in Figure 1 and Table 1.
6. Discussion
6.1. The Association between Cervical Spine Sprain and mTBI Signs and Symptoms. The 2012 Zurich consensus on concus-sion in sports led by McCrory et al. (2013) defined a list of 22 common symptoms of mTBI divided into 4 main categories, as described in Table 3 [4, 6, 11–13]. The majority of mTBIs (80–90%) are resolved in 7 to 10 days [4, 14, 15]. However, in the remaining 10 to 20%, symptoms may persist for more than 10–14 days, and even for several months after trauma [4, 16]. This clinical picture is diagnosed as PCS and the etiology for PCS is not well defined in the literature [11, 14, 17].
As mentioned previously, the most common symptom in subjects after mTBI is posttraumatic headache (PTH) [18, 19].
Table 1: Preliminary search of literature (total results/abstracts (Abs) selection/articles (Art) for review).
Date January 1, 1990, to February
16, 2014
February 16, 2014, to May 15, 2014
May 15, 2014, to May 19, 2015
Resources Keywords Total Abs Art Total Abs Art Total Abs Art
PubMed Concussion, Neck 180 12 8 10 0 0 21 5 1
PubMed TBI, Neck, Treatment 56 0 0 0 0 0 7 2 1
PubMed TBI, Cervical 83 0 0 33 0 0 17 0 0
PubMed Concussion, Chiropractic 12 4 1 2 0 0 2 0 0
PubMed Concussion, Physiotherapy 53 3 2 3 0 0 12 2 1
PubMed Concussion, Physical
Therapy — — — 138 4 1 38 6 1
PubMed Concussion, Athletic
Training, Cervical 30 2 2 0 0 0 6 1 0
ICL Concussion 32 2 2 0 0 0 4 1 1
SportDiscus Concussion, Neck 144 0 0 7 0 0 10 4 1
SportDiscus TBI, Neck, Treatment 5 0 0 0 0 0 0 0 0
SportDiscus Concussion, Neck,
Treatment 15 1 1 4 1 0 3 1 1
SportDiscus Concussion, Cervical 65 1 1 3 0 0 3 2 1
SportDiscus Concussion, Chiropractic 9 2 0 0 0 0 2 0 0
SportDiscus Concussion, Physiotherapy 34 2 2 0 0 0 7 2 1
SportDiscus Concussion, Athletic
Training, Cervical 13 1 1 0 0 0 1 1 1
CINAHL Concussion, Manipulation 3 3 2 0 0 0 2 1 1
CINAHL Concussion, Guideline 19 0 0 1 0 0 7 0 0
Cochrane Concussion 4 1 1 0 0 0 1 1 0
PEDro Concussion, Physical
Therapy 2285 11 5 0 0 0 0 0 0
PEDro mTBI, Physical Therapy 215 1 1 0 0 0 0 0 0
PEDro mTBI, Manual Therapy 99 0 0 0 0 0 0 0 0
PEDro Concussion, Manual
Therapy 1132 2 2 0 0 0 0 0 0
PEDro Concussion, Chiropractic 22 0 0 0 0 0 0 0 0
Total 4510 48 31 201 5 1 143 29 11
The incidence of PTH varies between 5 and 90% [16, 20]. Their prevalence in children with mTBI is from 73 to 93% [19]. The diagnosis of PTH can be difficult to address in subjects with a history of preexisting headaches. However, PTH syndrome diagnosis is considered when the intensity or frequency of headaches increases after trauma [19]. PTH is defined as a headache that occurs within 1 week after regain-ing consciousness or within 1 week followregain-ing head trauma [17]. The majority of PTH resolve within 6 to 12 months, and it is caused by cervical muscle tension and posture impairment [17]. Because headache is one of the major causes of morbidity in mTBI subjects, health care professionals should manage this symptom with a high level of priority [17].
Biologically, concussions usually resolve 7 to 10 days after trauma in adults [4, 21]. PCS related symptoms are nonspe-cific. Professionals must consider other pathologies as alter-native explanations to persistent symptoms [4, 17]. Mean-while, a recent study suggests that even at 1 month or more after concussion, the cerebral blood flow is decreased in 36%
of 11- to 15-year-old subjects who suffered mTBI compared to a nonconcussed control group [22]. Further studies are needed to clarify this phenomenon.
Rather than a structural problem, PCS would be related to a brain dysfunction problem [15]. This would explain the negative results on most of the medical imaging prescribed in emergencies [15]. In addition, a prospective Norwegian study of 348 participants identified through a questionnaire that headaches persisting for more than 3 months after trauma and diagnosed as PCS are often related to a musculoskeletal pathology. In other words, the head or brain injury does not cause the persistent symptoms [23]. These results show the importance of potential cervical impairment in patients with mTBI [4, 14, 16, 17].
6.2. Mechanism of Injury. Recent studies correlated mTBI with whiplash occurrence [12, 16, 24, 25]. Furthermore, Schneider et al. (2013) demonstrated in a prospective study with 3,832 male ice hockey players (11–14 years old) that
Original research 4,854 results
(keywords)
82 abstracts selected and read
43 articles (inclusion criteria)
14 articles “the association between cervical spine sprain and mTBI signs
and symptoms” 26 articles “mechanism of injury” 26 articles “treatments” Exclusion criteria 39 articles
34 articles did not match the three objectives of this study
(i) 2 case studies (ii) 2 magazine articles (iii) 1 expert comment
Figure 1: Research method for this review.
the presence of headache and neck pain in a preseason evaluation increases the risk of concussions during the season [26]. Consequently, a neck examination should be part of the postconcussion follow-up in addition to the neurological screening examination [6].
Whiplash is defined as a mechanism of acceleration-deceleration transferred to the cervical spine [6, 20, 27, 28] (see Table 4). With its large range of motion, the upper cervical spine is the most mobile part of the spine. During a whiplash, cervical structures are stressed at their end ranges of motion which can lead to neck injuries [29]. The impact generates stresses and injuries in the bones and soft tissues of the cervical spine, causing clinical manifestations [24]. Among those, whiplash symptoms include neck pain, cer-vicogenic headaches, chest pain, memory and concentration disturbances, muscle tension, sleep disturbances, dizziness, fatigue, cervical range of motion restrictions, irritability, tinnitus, and visual disturbances [12, 17, 20, 24, 25]. A preliminary study has demonstrated that low velocity impacts between 4 and 12 km/h can provoke neck and head injuries causing dysfunctions and pain [12]. These symptoms are often similar to those listed for mTBI, which leads to confusion for the medical community [12, 14, 16, 25].
The pathophysiology related to the patient’s symptoms originates from one or several structures of the cervical spine.
After a trauma involving the cervical region, the involvement of muscles, ligaments, arteries, nerves, the esophagus, the temporomandibular joint, intervertebral discs, zygapophysial joints, vertebrae, and the atlantooccipital joint creates a complex challenge for clinicians [16, 17, 20].
One of the hypotheses raised in the literature for the origin of neck pain is the involvement of the cervical zyga-pophysial joints [30]. Zygazyga-pophysial joints have been shown to be the source of neck pain, headaches, visual distur-bances, tinnitus, and dizziness in patients who have sustained whiplash [14, 24, 25]. In this following order, the C1-C2, C2-C3, C0-C1, and C3-C4 levels are the most often described in association with cervical symptoms following mTBI [16, 24, 26, 31]. More specifically, cervical zygapophysial joint pain is expressed by a hypersensitivity and hyperexcitability of the spinal cord reflexes, causing an increase of nociceptive pro-cesses in the central nervous system [32]. The cross-sectional study of Smith et al. (2013) recruited 58 adults (18–52 years old) with chronic whiplash disorder and provided a facet joint block to all participants [32]. They analyzed characteristics of responders and nonresponders to facet joint block and concluded that patients with chronic Whiplash-Associated Disorder (WAD) show similar sensory disturbances, motor dysfunction, and psychological distress [32]. Another study published by Treleaven et al. (1994) supports the implication
T a ble 2: Inc luded st udies d es cr ip ti o n . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Be ck er [3 4 ] This re vie w w as de ve lo p ed as p ar t o f a d eb at e and ta ke s the “p ro ” st ance tha t ab n o rma li ti es o f st ru ct ur es in th e n ec k ca n b e a significa n t so u rc e o f h ea dac h e A d ul t L it era tur e re vie w (i) C linical tr ea tm en t tr ials in vo lv in g p at ien ts w it h p ro ven p ainf u ldis o rd er s o f u p p er cer vica l zyga p o p h ysial jo in ts h av e sho wn significa n t h ea dac h e re lief wi th tr ea tm en t dir ec te d at cer vical p ai n genera to rs (ii) H eadac hes rela ted to cer vica ls p ine dis o rd er s (cer vicog enic he adac he an d chr o nic he adac he at tr ib ut ed to w h ipl as h in ju ry ) re m ai n o n e of th e m o st co n tr o ve rs ia la re as o f he adac he medicine (iii) Dia gnost ic cr it er ia fo r cer vicog enic he adac he ha ve b een de ve lo p ed by the CHISG Bo gd u k [3 0 ] T o summa rize the ev idence tha t im p lica tes th e cer vica l zyga p o p h ysial jo in ts as the le adin g so u rc e o f chr o nic nec k pa in aft er whi p la sh Ad u lt N ar ra ti ve re vie w D at a we re re tr ie ve d from st udies tha t addr ess ed th e p o stm o rt em fea tu re s an d b io mec h anics o f in ju ry to th e cer vical zyga p o p h ysial jo in ts and fr o m cl inical st udies (i) C linical st udies h av e sho wn th at zyga p o p h ysial jo in t pa in is ve ry co mmo n am o n g p at ien ts w it h chr o nic nec k pa in aft er whi p la sh (ii) The fac t th at m u lt ip le lines o f evidence ,usin g indep enden t tec hniq ues, co n sist en tl y im p lica te the cer vical zyga p o p h ysial jo in ts as a si te o f in ju ry an d so ur ce o f pa in st ro n gl y im p lica tes in ju ry to th es e jo in ts as a co m mo n b asis fo r chr o nic nec k pa in aft er w h ip lash Bo n k et al .[ 38 ] T o ev al ua te th e eff ec ti veness o f co n ser va ti ve ma nag emen t fo r ac u te W hi p lash-A ss o cia ted Dis o rd er Ad u lt Sy st ema tic re vie w an d met a-a na lysis o f ra n d o mized co n tr o lled trial s Im p ro vemen t o f cer vical m o vemen t in the ho ri zo n ta l pl an e sho rt ter m co u ld b e p ro mo te d by the us e o f a co n ser va ti ve in te rv en ti o n .Th e u se o f a b eha vio ra l in te rv en tio n (e .g., ac t-as-usual ,e d u ca tio n ,a nd se lf-ca re inc ludin g regula r ex er cis e) m ay b e an eff ec ti ve tr ea tm en t in red ucin g p ai n and im p ro vin g cer vical mob ili ty in p at ien ts wi th ac u te W AD II in th e sho rt-medi um te rm Bo ri ch et al .[ 2] In th is sp ecia li n ter est ar tic le ,w e dis cuss the defini ti o n an d risk fac to rs ass o cia te d w it h co nc ussio n ,s umma rize and hig hlig h t so me o f th e m ost w id ely us ed ass ess me n t to ols , an d cr it iq u e the ev idence fo r cu rr en t p ri n ci p le s o f co n cu ss io n ma nag emen t A d ul t L it era tur e re vie w (i ) D is ea se C o n tr o la n d P rev en ti o n d esc ri be s mi ld tr au ma tic br ain in ju ry (m TBI w hic h inc ludes co nc ussio n ) as a silen t ep idemic (ii) An est ima te d 1.6 millio n to 3.8 millio n sp o rt -and re cr ea ti o n -r ela ted b ra in in jur ies o cc ur in th e U ni te d St at es an n u al ly ,a n d u p to 75 %a re cl as si fi eda sm il d (iii) “Rest” in th e fo rm o f d ela yin g ret ur n to co m p et it iv e sp o rts ma y b e b et te r ser ve d by a uni ve rs al p er io d o f 7 to 10 d ay s th an by sy m p to m m on it or in g ,pr im ar il y to pre ve n t th e p o te n ti al for re in ju ry
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Brol in so n [7 ] T o syst ema ticall y re vie w th e ev idence fo r re st, tr ea tmen t, and re h abi li ta ti on aft er sp or t-re la te d co nc ussio n Sp or ts Ad u lt P edia tr ic Sy st em at ic re vi ew (i ) F ro m 74 9 ar ti cl es ev al ua ti n g re st an d 1, 17 5 ev al ua ti n g tr ea tm en t, 2 st udies m et cr it er ia fo r the eff ec t o f rest an d 10 ab str ac ts m et cri te ria fo r tr ea tm en t. Th ree fu rt her tr ea tmen t ar ti cl es w er e iden tified by the au th o rs (ii) H eal th p ro fessio n als ar e mo re in vo lv ed in sp o rts an d in the co nc ussio n s fol lo w-u p (iii) In te rv en ti o n s inc luded m an ual sp inal thera p y, p h ysio th era p y, an d n eur o mo to r and se n so rimo to r re tr ainin g co m pa re d w it h rest and grad ua te d ex er cis e, for u p to 8 we ek s Co ll in s et al .[ 43 ] T o de ve lo p and valida te a cost-effe ct ive to o lt o m ea sur e nec k st re n gt h in a hig h sc h o o l se tt in g and to det er mine if an th ro p o met ric me asur emen ts ca p tur ed by A T s ca n p redic t co nc ussio n ri sk 6,7 0 4 hig h sc h o o l at h let es in b o ys ’a nd gi rls ’s o ccer , ba sk et ball ,a n d lacr oss e Fe as ib il it y st u d y Pi lo t stu dy (i) D iff er ences in o vera ll n ec k st ren gt h m ay b e us ef u lin de ve lo p in g a scr eenin g to o lt o d et er mine w hic h hig h sc ho o la thlet es ar e at hig her risk o f co n cu ssio n. Once iden tified ,t h es e at h let es co u ld b e ta rg et ed fo r co n cu ss ion pre ve n ti on pro gr ams E ckner et al .[ 4 0 ] The p u rp os e o f this st u d y was to det er mine the infl uence o f n ec k st re n gt h an d m us cl e ac ti va tio n st at us o n re su lt an t h ea d kinema ti cs aft er im p u lsi ve loadin g 4 6 co n tac t sp o rt at h let es 24 ma les; 22 fe ma les age d 8 to 30 ye ars D es cr ipt iv e lab or at or y st ud y (i) N ec k st ren gt h and im p ac t an ti ci p at io n ar e 2 p o te n ti al ly m o d ifi abl e ri sk fa ct or s for co n cu ss ion (i i) Th e re su lt so ft h iss tu d y su gg es tt h atg re at er n ec k st re n gt h at te nu at es th e h ea d ’s d yn am ic re sp o n se to ext er n al fo rces Fe rn ´andez D e L as Pe ˜nas et al .[2 4] Th e ai ms of th e p re se n t p ap er are to det ail a m an ual ap p ro ac h de ve lo p ed by o ur re se ar ch gr o u p , to hel p in fu tu re st udies o f the ma nag emen t o f th e se q uels to w h ip lash in ju ry ,a nd to sug gest expl an at io ns fo r the me cha n isms of th is prot o col A d ul t L it era tur e re vie w (i) Th e clinical syndr o me o f w h ip lash in ju ry inc ludes nec k p ain, u p p er tho racic p ain, cer vicog enic he adac he , ti gh tn ess, dizziness, rest ric ti o n o f cer vica lr an ge o f mo ti o n ,t inni tu s, an d b lu rr ed visio n (ii) Sp inal ma ni p u la ti o n /mo b iliza tio n and so ft tissue mo b iliza ti o n te chniq ues ar e ma n u al th era p ies co mmo n ly us ed in th e m an ag emen t o f n ec k d is o rder s
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs K enned y [1 4 ] This d o cumen t is in tended to p ro vide th e u se r w it h in st ruc ti o n an d dir ec ti o n in th e re h abi li ta ti on of P C S O n ta ri o H o spit al Ca n ad a Ad u lt PCS and tr ea tmen t guidelines (i) C er vicog enic (ii) A u to no mic (iii) V est ib ula r (i v) V isio n (v ) E du ca ti on (i) A na to micall y, the cer vical sp ine is cl os el y link ed to st ru ct u re s th at ca n cau se m any o f th e sa m e sy m p to m s as co nc ussio n (ii) PCS tr ea tmen t has tradi ti o n all y co n sist ed o f rest, ed uca tio n, neur o cogni ti ve re ha b ili ta ti o n ,a nd an tidep ress an ts w it h limi te d eff ec ti veness (iii) B ala nce d efici ts an d p ost u ral in st ab ili ty ar e co mmo n ly re p o rt ed aft er co nc ussio n Gr av el et al .[ 36 ] This syst ema ti c re vie w in ve st iga ted th e eff ec ti veness o f in te rv en ti o n s ini ti at ed in ac u te se tt in gs fo r p at ien ts w ho exp er ience m T BI Ad u lt Sy st em at ic re vi ew Co ch ra n e’ s ri sk o f b ia s ass essmen t to ol (i) A cco rding to the p u blishe d li tera tur e, no in te rv en ti o n ini ti at ed ac u tel y h as b een cl ea rl y ass o cia te d w it h ap o si ti veo u tc o m e fo rp at ie n tsw h o su st ai nm T B I, an d ther e is li tt le ev idence sug ge st in g tha t fo llo w-u p in te rv en ti o n s m ay b e ass o cia ted wi th a b et te r o u tco me (ii) Ther e is a p au ci ty o f w ell-designed clinical st udies fo rp at ie n tsw h o su st ai nm T B I. Th e la rg ev ar ia b il it y in o u tc o m es me asur ed in st udies limi ts co m p ar is o n be tw ee n th em G u skie wicz et al . [9] T o re vi ew th e cu rre n t li te ra tu re to iden tif y the most se nsi tive and re lia b le co nc ussio n ass essmen t co m p on en ts for in clu si on in th e re vi se d ve rs ion :t h e SC A T 3 A d ul t L it era tur e re vie w (i) O ne o f th e m aj o r ch allen ges in th e m edical ma nag emen t o f co nc ussio n is th at th er e is n o sing le “g o ld st anda rd” fo r ass essin g an d d ia gnosin g the in ju ry (ii) B ala nce d efici ts o r in st ab ili ty ar e o ft en o b se rv ab le in p at ien ts fol lo w ing co n cu ssio n and th e p re se nce o f thes e defici ts m ay b e an indica to r o f ve st ib ula r disr u p ti o n Ha n so n et al .[ 6 ] Th e p u rpo se o f th is art ic le is to re vi ew th e cu rre n t li te ra tu re in th e m an ag emen t and p re ven ti o n of co n cu ss ion Pe d ia tr ic s R ev ie w (i) Th e ris e in the n u m b er o f co nc ussio n di ag nos es m ay b e d u e, in p ar t, to incr eas ed aw ar eness rega rdin g the p o te n tial fo r co m p lica ti o n s o f co n cu ssio n s an d seq uelae of m u lt ipl e co n cu ss ions ,a s opp o se d to an ac tu al incr ea se in th e incidence o f co n cu ssio n alo ne (ii) T yp ical sign s an d sym p to m s o f co n cu ssio n
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Ha rm o n et al .[ 5] T o p ro vide an ev idence-bas ed , b est p rac ti ces summa ry to assist p h ysicia n s wi th th e eval u at io n an d m an age m en t o f sp o rt s co nc ussio n Ad u lt Ch il d re n St at emen t o f the Amer ica n M edical So ciety fo r Sp o rt M edicine R ev ie w (i )H o w ev er ,a sm an ya s5 0 % o f th ec o n cu ss io n s m ayg o unr ep o rt ed (ii) H eadac he is th e m ost co m mo n ly rep o rt ed sym p to m wi th d iz zi n es s th e sec o n d m o st co m m o n H eadac he C lassifica tio n C o mmi tt ee o f th e In te rn at io nal H eadac he So ciety (IHS) [3 3] The In te rn at io nal C lassifica tio n o f H eadac he Dis o rd er ma y b e re p ro d uced fr eel y fo r scien tific, ed uca tio nal ,o r cl inical us es by in st it u tio n s, so ciet ies, o r indi vid u als Ad u lt Ch il d re n Review guideline (i) C er vicog enic he adac he fr o m (1 ) migra ine and (2 )t en si o n -t yp e he adac he inc ludes side-lo ck ed p ain, p ro vo ca tio n o f typ ical he ad ache by dig it al p ressur e o n ne ck m u sc les and by he ad mo vemen t, and p o ster io r-to-a n ter io r radi at io n o f pa in (ii) Dia gnost ic cr it er ia He ch t [1 6 ] This ar tic le re vie w s the li te ra tu re o n ma nag emen t o f p o st tr au ma ti c he adac hes, p res en ts an ap p ro ac h to th e ass essmen t and tr ea tm en t o f indi vid u als w it h h ea dac h es fo ll ow in g T B I th at ap p ea r to b e cer vicog enic, fo cus es sp ecifical ly o n iden tif yin g o cci p it al neura lg ia, an d d is cu ss es th e te chniq ue o f o cci p it al n er ve bl o ck s 7m al es (1 8– 4 2 yo ) 3 fema les (22–6 4 yo ) Ret rosp ec ti ve re vie w & Rep o rt o f te n p at ien ts (i) W hile th er e ar e a va riety o f diff er en t p ost tra uma tic he adac hes, cl inicia n s m u st b e aw ar e o f all p o te n tial p res en ta ti o n s inc ludin g thos e ema n at in g fr o m the cer vical sp ine an d its affi lia ted st ru ct ur es (e .g., cer vicog enic) (ii) In ju ry to th es e st ruc tu re s (inner va te d by aff er en t fib re s o f the 3 su p .cer vi ca lr o o ts) (iii) Thes e inc lude b u t ar e no t limi te d to m us cl es, liga men ts, ve ss els, so ma tic and sym p at hetic n er ve s, es oph ag u s, te m p orom an d ibu la r joi n t, d is cs , zyga p o p h ys ea lj o in ts, cer vical ver te b rae ,a nd th e at la nt o ax ia lc o mp le x (iv) W h ip la sh sy ndr o me ma y b e the p rima ry fac to r in ma n y p o st co nc ussi ve he adac hes H ynes and Dick ey [12] T o exa mine the re la ti o n shi p be tw ee n th e oc cu rr en ce o f W h ip la sh -A ss o cia te d D is o rder s an d con cu ss io n sy m pt oms in ho ck ey pl ay ers Hi gh sc h o o l, co ll eg e/uni ve rs it y, On ta ri o H o ck ey L eague, and men ’s re cr ea ti on al te ams (15–3 5 yo) 20 te am s Pro sp ec tive stu dy (i) 18 3 p la yer s w er e reg ist er ed fo r th is st ud y; 13 re cei ve d ei th er a m ec ha nical w h ip lash in ju ry o r a co n cu ssio n in ju ry (i i) Th er e is a str o n g as soc ia ti o n be tw ee n w h ip la sh-ind uce d ne ck in ju ri es an d the sy m p to ms o f co nc ussio n in ho ck ey in ju ri es (iii) A ccelera ti o n an d d ecelera tio n o f the he ad an d n ec k co m p lex o cc ur s in sp o rt s and ca n p o ten ti al ly cr ea te in ju ri es simila r to thos e inc u rr ed in lo w velo ci ty m o to r ve hic le acciden ts, as st at ed in a recen t li tera tur e re vie w fo cu sed o n W h ip la sh -A ssoc ia ted D iso rd er s
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Ki ng et al .[ 35 ] The o b jec ti ve w as to det er mine th e sen si ti vi ty ,s p ecifici ty ,a n d li ke li ho o d ra ti o o f m an ual exa mina tio n fo r th e d ia gnosis o f cer vical zyga p o p h ys ea lj o in t p ain 17 3 p at ien ts w it h n ec k pa in in w h o m cer vical zyga p o p h ys ea lj o in t pa in w as su spect ed Retr os p ecti ve st u d y (i) M an ual exa mina tio n h ad a hig h sen si ti vi ty fo r cer vical zyga p o p h ys ea lj o in t p ain, at th e seg men tal le ve ls co mmo n ly sym p to ma ti c, b u t its sp ecifici ty w as poo r (ii) The p res en t st u d y fo und m an ual exa mina tio n o f the cer vi ca ls p ine to la ck va lidi ty fo r the di ag nosis o f cer vical zyga p o p h ys ea lj o in t p ain Ko zl o w sk i et al .[ 3] T o ass ess ex er cis e in to lera nce in male an d female p at ien ts w it h PCS 34 p at ie n ts (P C S) 17 ma le s, 17 fe ma le s Ag e = 25 .9 ± 10.9 22 unin ju re d indi vid u als Cr os s-s ec tio nal st u d y (i) Sym p to m s fr o m co n cu ssio n typ icall y re so lv e w it hin 7t o1 0d ay s (ii) The defini ti o n o f PCS gi ven by th e W o rld H eal th Or ga niza tio n inc ludes a hist o ry o f tra uma tic b ra in in ju ry an d 3 o r mo re sym p to m s (iii) N o cogni ti ve test in g ,e xc lu sio n o f o ther d is o rder s, o r sy m p to m thr eshold exists fo r the di ag nosis o f P CS (i v) P at ien ts wi th PCS h ad a sym p to m -limi te d resp o n se to ex er cis e, and th e tr eadmi ll te st was a p o te n tial ly us ef u lto ol to mo n ito r the re co ve ry fr o m P C S Kr is tj anss on an d Tr el ea ve n [2 9] The p u rp os e is to re vie w dizziness in nec k pa in: im p lica tio n s fo r ass essmen t and ma nag emen t A d ul t R ev ie w (i) D ist u rb an ces to th e aff er en t in p u t fr o m the cer vical re gi on in th o se w it h n ec k p ai n m ay b e a p o ss ibl e ca u se o f sym p to m s suc h as dizziness, u n st eadiness, an d visual dist urba nces, as w ell as sign s o f al te re d p ost u ral st ab il it y, cer vica lp ro p rio cep ti o n ,a nd he ad an d ey e mo vemen t co n tr o l Led d y et al .[ 27 ] The ob je ct ive w as to co m p ar e sym p to m s in pa tien ts wi th p h ysio logic p o st co nc ussio n dis o rd er (PCD) ver sus cer vicog enic/v est ib u la r P CD 12 8 adu lt s Ret rosp ec ti ve re vie w Quest io n na ir e (i) C linicia n s sho u ld co n sider sp ecific te st in g o f ex er cis e to lera nce and p er fo rm a p h ysical exa mina tio n o f the cer vi ca ls p ine an d the vest ib u la r/o cu la r systems to det er mine the et io log y o f p ost co n cu ssio n sym p to m s (ii) C o nco m it an t in jur y to the cer vical sp ine re se m b lin g w h ip lash ma y o cc ur as a resu lt o f the accelera ti o n , decelera ti o n fo rces sust ai ned in co n cu ssi ve tra uma (iii) St ru ct ural an d func tio nal in jur y to the cer vical sp ine ca n b e ass o cia ted wi th p ro lo n ge d sym p to m s suc h as he ad ache, dizziness, b lu rr ed vi sio n ,a nd ver tigo
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Led d y et al .[ 4 4 ] This re vie w fo cus es o n re h abi li ta ti on of co n cu ss ion an d p o stco nc ussio n sy ndr o me Ad u lt Ch il d re n Review (i) E ar ly ed uca tio n, cogni ti ve b eha vio ral thera p y, and aer ob ic ex er cis e th era p y h av e sho wn efficac y in cer ta in pa ti en ts b u t h av e limi ta ti o n s o f st u d y design L eslie an d C ra to n [2 5] B as ed o n the cu rr en t m edical ev idence ,w e w o uld sug ge st th at th e cons te ll at ion of sy m p to ms p res en tl y d efined as co n cu ssio n d o es n o th av et oi n vo lv et h e b ra in A d ul t E di to ri al co mmen t (i ) C on cu ss io n sy m ptoms can em an at e from th e cer vical sp ine (ii) W h ip lash mec h an ism s o f in ju ry ar e iden tical to th e “im p u lsi ve fo rces” d es cr ib ed in co nc ussi ve in ju ri es (iii) N o ta b ly ,s ym p to m s suc h as h ea dac h e, nec k pa in, dist urba nce o f co n cen tr at io n o r m emo ry ,dizziness, ir ri ta b ili ty ,s leep dist urba nce ,a n d fa tigue ha ve b een des cr ib ed in b o th co n cu ssio n and w h ip lash pa ti en ts (i v) C er vical zyga p o p h ysial jo in ts h av e b een im p lica te d as genera to rs o f he ad ache an d dizziness (v) Th e o ve rla p wi th nec k /w hi p lash in jur ies is eviden t Lu ca s [1 9] This ar tic le re vie w s the li te ra tu re o n he ad ache ma nagemen t in co nc ussio n an d m TBI Ad u lt P edia tr ic Un it ed St at es L it er atu re re vi ew (i) R ep o rts o f he adac he aft er co nc ussio n o r m T BI in ch il d re n ra nge d fr o m 72 % to 93 % (ii) H ead ache is o n e o f the most co mmo n sy m p to ms aft er T B I an d P T H m ay b e p ar t of a cons te ll at ion of sym p to m s th at is se en in th e p ost co n cu ssi ve syndr o m e Ma kd is si et al .[ 8] The ob je ct ives o f th e cur re n t p ap er are to re vi ew th e lit er at u re re ga rdin g diffic ul t co n cu ssio n an d to p ro vide re co mmenda ti o n s for an appro ac h to the in ve st iga tio n and ma na ge men t o f pa tie n ts wi th pe rs is te n t sym p to m s Ad u lt Sp or t Quali ta ti ve re vie w (i) C as es o f co nc ussio n in sp o rt w her e cl inical re co ve ry falls o u tside th e exp ec te d w indo w (i .e ., 10 d ay s) sho u ld b e ma nag ed in a m u lt idis ci p lina ry ma nner by he al th ca re p ro vider s wi th exp er ience in sp o rts-r ela ted co nc ussio n M ar shall [11] This p ap er is a re vie w o f recen t li te ra tu re on th e topi c of co n cu ss ion ,c ons is ti n g o f b io m ec ha nics, pa th o p h ysio log y, dia gnosis, an d sideline ma nag emen t A th let es Un it ed St at es N ar ra ti ve re vie w (i) Th e cer vi ca ls p ine no t o n ly is a p o ten ti al so u rc e o f in ju ry th at w e m u st b e aw ar e o f b u t als o is im p lica ted as a fac to r in the co nc ussio n it se lf (ii) Sig n s and sy m p to ms o f co nc ussio n fr o m th e A ss o cia tio n o f Sp o rt C o lleg e o f M edicine (A C SM ) up d at ed cons ens u s st at em en t Mau ga n s et al .[ 22 ] The go al o f th is in ve st iga tio n w as to exp lo re cer eb ra lb lo o d flo w flu ct u at ion aft er p ed ia tr ic sp or t-re la te d con cu ss io n Tw el ve ch il d re n A ges 11 to 15 ye ar s C o n tro lg roup C linical st ud y (i) St at ist icall y significa n t al tera tio n s in cer eb ral b lo o d flo w w er e d o cumen te d in the sp o rt-r ela te d co n cu ssio n gr o u p ,wi th re d u ct io n in cer eb ral b lo o d flo w pre d om in at in g. Im prove m en t tow ard con tr ol va lu es o cc u rr ed in o n ly 27 % o f the pa rt ici p an ts at 14 da ys an d 64 % at > 30 da ys aft er sp o rt-r ela te d co n cu ss io n
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Mc C ro ry et al .[ 4 ] The ne w 201 2 Z ur ich C o n se nsus st at emen t is d esig ned to b ui ld o n th e p ri nci p les o u tline d in the p re vio us do cu men ts and to de ve lo p fur th er co ncep tu al under st andin g o f this p ro b lem usin g a fo rm al co n sen sus-b as ed ap p ro ac h In te rn at io nal co n sen sus (i ) A du lt s (ii) P edia tr ic In ter n at io na lc o n se nsus Sp or t con cu ss io n (i) A n ini ti al p er io d o f re st ma y b e o f b enefi t (ii) M u lt imo d al p h ysio th era p y tr ea tmen t fo r indi vid uals wi th cl inical ev idence o f cer vical sp ine an d/o r ve st ib ula r d ysf unc tio n m ay b e o f b enefi t (iii) P er sist en t sym p to m s (> 10 d ays ) ar e gener al ly re p o rt ed in 10 –15% o f co nc us sio n s. In ge neral , sy m p to ms ar e n o t sp ec ifi c to co nc uss io n and it is im p o rt an t to co n sider o th er pa th o logies (i v) PCS sho uld b e m an ag ed in a m ul tidis ci p lina ry ma nner by he al th ca re p ro vider s wi th exp er ience in sp o rts co nc uss io n Mi ha li k et al. [3 9] The ob je ct ive w as to ev al u ate th e eff ec t o f cer vica lm us cl e st ren gt h o n he ad im pac t b io m ec ha nics 37 volu n te er ic e ho ck ey pl ay ers Ag e = 15 .0 ± 1.0 ye ar s Pr o sp ec tive cohor t stu dy (i ) Th e h yp o th es is th at p la ye rs wi th gr ea te r sta ti c n ec k st re n gt h w o u ld exp er ience lo w er re su lt an t h ea d accelera ti o n s w as no t su p p o rt ed (ii) Ther e is st ill no nem p ir ical su p p o rt fo r th e ro le n ec k mu sc u lat u re m ay p lay in re d u ci n g th e ri sk o f m il d T B I th at is w o rt h y o f in ve st iga tio n in a yo un g at-r isk sa m p le Mo se r et al .[ 21 ] The o b jec ti ve o f this ar tic le is to ev al ua te th e efficac y o f cogni ti ve an d p h ys ic al re st for th e tr ea tm en t o f co n cu ss io n Hi gh sc h o o la n d co ll eg ia te at h let es (𝑁=4 9) Ra n ge = 14 – 23 yo Me an = 15 .0 yo 67% m ale 33 % fe m al e Retr os p ecti ve an al ysi s (i) P ar ti ci pa n ts sho w ed significa n tl y im p ro ve d p er fo rma nce o n Immedia te P o st-C o n cu ssio n A ss essmen t an d C ogni ti ve T est in g and decr ea se d sym p to m rep o rt in g fo llo w in g p re sc ri b ed cogni ti ve an d ph ys ic al re st (ii) Thes e p relimina ry d at a sug ge st th at a p er io d o f cog n it iv e and ph ysic al re st ma y b e a us ef u lme an s o f tr ea ti n g co n cu ssi o n -r el at ed sym p to m s, w h eth er ap p li ed so o n afte r a co n cu ss io n o r w ee k s to mo n ths la te r P ellet ier [18] The p u rp os e o f this p ap er is to p res en t a re vie w o f th e d iag n osis an d tre at m en t of th e p ote n ti al ly ca ta st ro p hic nec k an d h ea d in ju ri es ca u sed by sp ea ri n g in C an ad ian am at eu r fo o tb al l Ama teur fo o tb al l Un it ed St at es an d Ca n ad a L it er atu re re vi ew (i) A ss o ci ate d cer vi ca lt ra uma w it h co n cu ss io n m ay inc lude o n e o r se veral o f nec k pa in, re d u ced cer vical ra n ge o f m o vemen t, cer vicog enic he adac he , cer vicog enic ve rt ig o, an d o cci p it al neuralg ia (ii) Se ve ral m an ual tec hniq ues fo r th e tr ea tmen t o f p o st tr au ma ti c co n cu ssio n syndr o m e h av e b een des cr ib ed as ei ther “dir ec t” o r “indir ec t” Reid et al .[ 37 ] This st u d y ai med to d et er mine th e efficac y o f sust ained na tu ral ap o p h ys eal gl ides (S N A G s) in th e tr ea tm en t o f th is co n d iti o n 34 ad u lt s 17 SN A G s 17 Placeb o D o ub le-b lind ra n d o mized co n tr o lled cl inical tr ial (i) Th e SN A G tr ea tmen t had an immedia te cl inicall y an d st at ist icall y significa n t sust ained eff ec t in red ucin g dizziness, cer vica lp ain, an d d is ab il it y ca u se d by cer vical d ysf u nc ti o n
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Sc hmid t et al .[4 2] The p u rp os e o f this st u d y was to co m p ar e the o d ds o f sust ainin g hig her m ag ni tude in-s eas o n he ad im p ac ts b etw een at h let es wi th hig her and lo wer p re se as o n p er fo rma nce o n cer vi ca lm us cle ch ar ac te ri st ics 49 hig h sc h o o la nd co ll eg ia te Amer ica n fo ot b al lpl ay er s C o ho rt st ud y (i) Th e st u d y findin gs sho w ed th at gr ea te r cer vical st iff ness an d less an gu la r disp lacemen t aft er p er turba ti o n re d u ced the o d ds o f sust ainin g hig her ma gni tude he ad im pac ts; ho w ev er ,t h e fi ndin gs did no t sho w th at p la yer s w it h st ro n ge r and la rg er nec k m u sc les mi ti ga te he ad im pac t se ve ri ty (ii) M ale at h let es al so exhib it gr ea ter st iff ness an d ca p aci ty to st o re elast ic ener gy co m p ar ed wi th fe male at h let es Sc hneider et al . [26] The o b jec ti ve o f this st u d y was to det er mine the ri sk o f co nc ussio n in yout h m al e h o cke y p la ye rs w it h pre se as o n re p or ts of n ec k pa in, he adac hes, an d/o r dizziness 38 32 m al es Ic e h o ck ey p la ye rs (11 –1 4 yo) 280 tea m s Pro sp ec tive stu dy (i) P re se as o n re p o rt s o f n ec k p ai n and he ad ache wer e ri sk fa ct or s for co n cu ss ion (ii) Dizziness was a ri sk fac to r fo r co n cu ssio n in the P ee W ee n o n bod y ch ec k in g (iii) A co m b ina ti o n o f an y 2 sym p to m s was a ri sk fac to r in th e P ee W ee n o n b o d y chec k in g co h o rt and th e Ba n ta m co h o rt (i v) N ec k pa in is th e thir d m ost co m mo nl y rep o rt ed b as el in e sy m p to mi nv ar si ty at h le te s Sc hneider et al .[10] The o b jec ti ve o f this st u d y was to det er mine if a co m b ina tio n o f ve st ib u lar reh abi li ta ti on an d cer vica ls p ine p h ysio th era p y decr ea se d the ti me un ti lm edical cle ara nce in indiv id u als w it h prol onge d p o st con cu ss io n sym p to m s 18 ma les 13 fe males 12–3 0 yea rs R an d o mized co n tr o lled trial (i) A co m b ina tio n o f cer vical and ve st ib u la r ph ysio th era p y d ec re as ed ti me to me dic al cle ara nce to re tu rn to sp o rt in yo u th an d yo u n g ad ul ts wi th p er sist en t sym p to m s o f dizziness, n ec k p ain, an d/o r he adac hes fo llo win g a sp o rt -r ela ted co nc ussio n (ii) The cer vical sp ine is ci te d as a so ur ce o f pa in in indi vid u als w it h w hi p lash (iii) The u p p er cer vical sp ine ca n ca u se cer vicog enic he adac hes (i v) A co m b ina ti o n o f ma n u al th era p y and ex er cis e has b ee n sh o w nt ob em o ree ff ec ti vet h anp as si ve tr ea tm en t mo dali ti es in indi vid u als w it h n ec k p ai n Sc o rza et al .[ 13] C ur re n t co ncep ts in co nc ussio n C h il dr en ado les cen ts L it era tu re re vie w (i) Ini ti al ev al ua ti o n in vo lv es elimina tin g cer vical sp ine in ju ry an d ser io us tr au ma ti c b ra in in ju ry (ii) Se lec ted sym p to m s o f co nc ussio n
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Si gn o ret ti et al .[ 15] The fo llo w in g re vie w rep re se n ts th e aut h o rs ’e ffor t to pi ec e to ge th er th e cur re n t co ncep ts an d the most re cen t fi ndings ab out the co m p le x b as ic p h ysio log y u nderl yin g the in ju ry p ro ce ss eso ft h isp ar ti cu la rt yp e o f b ra in tra uma and to em p h asize th e n ua nces in vo lv ed in co nd uc ti n g re se ar ch in th is ar ea E u ro p ea n co un tr ies Un it ed St at es Ad u lt L it er atu re re vi ew (i ) P o st con cu ss iv e sy m pt oms m ay b e prol onge d in a small p er cen ta ge o f cas es, b u t the ac u te clinical sy m p to ms la rgely refle ct a fu nc ti o n al dist urb ance ra ther th an a st ruc tu ral in jur y, w hic h u suall y is co nfir med by th e abs ence o f ab no rm ali ties o n st anda rd n eur o ima gin g st udies (ii) The sym p to m s o f co nc ussio n re flec ted a func tio nal dist urba nce ra ther tha n a st ru ct ural da ma ge suc h as co n tusio n, hemo rr hag e, o r lacera tio n o f the b ra in Sm it h et al. [3 2] This p re limina ry st u d y exa mined a sa m p le o f indi vid uals w h o did an d did no t resp o nd to facet b lo cka sw el la sh ea lt h y co n tr o ls to det er mine w het h er th er e w er e diff er ences in th eir p h ysical and psy cho logical fe at ur es o n ce th e eff ec ts o f th e b lo ck s h ad ab at ed an d sy m ptoms h ad re tu rn ed 58 ad ul ts (1 8–6 5 yo ) Cal ga ry ,Ca n ad a Cr os s-s ec tio nal st u d y (i) F o llo win g FB p ro ced ur es, b o th W AD gr o u ps demo nst ra te d genera lize d h yp ers ensi tiv it y to al l sen so ry tes ts, d ecr ea sed n ec k R O M, an d in cr ea sed su p er fi cial m u sc le ac ti vi ty wi th th e C CFT co m p ar ed to co n tr o ls (ii) B o th W A D gr o u p s d emo n st ra te d p sy ch o logical dist re ss (iii) C h ro nic W A D resp o nder s and no nr esp o nder s to feedbac k (FB) p ro ced ur es demo n st ra te a simila r pre se n ta ti on of se ns or y d is tu rb an ce ,m ot or d ysf unc tio n, an d p sy ch o logical dist re ss. H ig her le vels o f pa in ca ta st ro p hiza tio n and gr ea te r m edica tio n in tak e w er e th e o n ly fac to rs fo und to diff er en ti at e thes e gr o u ps Sp it zer et al .[ 28 ] The p u rp os e w as to exp o se th e cl inical cl assifica tio n o f W h ip la sh -A ss o cia te d D is o rder s A d ul t G uideline (i) G rades 0 to 4 (c linical p res en ta ti o n ) St ov n er et al .[ 23 ] A m ai n o b jec ti ve o f th is st ud y was to ass ess the validi ty o f th is dia gnosis by st u d yin g the he adac he p at ter n o f co n cu ss ed pa ti en ts th at pa rt ici p at ed in o n e hist o ric (𝑛 = 131 )a n d o n e pro sp ec ti ve coh or t (𝑛 = 217 ) st ud y 20 0 p at ien ts (18–67 yo ) T ra u ma in vo lv in g LO C o f< 15 min. Ka u n as ,L it h u an ia Quest io n na ir es st ud y (a ft er 3 mo n th s & 1 ye ar ) (i) E xist ence o f p ret ra uma tic he adac he was a p redic to r of p o st tr au m at ic h ea d ac h e, al th ou gh pre tr au m at ic he adac he se em s to h av e b een u nder re p o rt ed am o n g the co nc uss ed p at ien ts (ii) This is n ega ti ve co rr ela ti o n ,a nd th e lac k o f sp ecifici ty indica tes th at he adac he o cc u rr in g 3 m o n th s o r mo re aft er co nc ussio n is no t ca u se d by the he ad o r b ra in in jur y (iii) R at h er it ma y rep re se n t an ep is o d e o f o ne o f th e pr im ar y h ea d ac h es ,p o ss ibly in du ce d by th e st re ss of th e situ at ion
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Ta to r et al .[ 1] This rep o rt is in tended to im p ro ve u nder st an din g o f the ep idemio log y o f n eur o logical co ndi tio n s an d the eco n o mic im p ac t on th e C an ad ia n h ea lt h ca re sys tem an d so ciety Ad u lt Ch il d re n Ca n ad a St at is ti ca lr ep or t (i ) C er eb ra lc on cu ss io ns are com m o n ly k n o w n as m il d tra u ma tic b ra in in ju ry (m TBI) (ii) B y co n trast, St at ist ics C an ada est ima ted in re cen t st udies tha t the an n u al incidence fo r m T BI is 6 0 0 p er 10 0 ,000 pe rs o n s an d 11 .4 p er 10 0 ,000 in h ab ita n ts fo r a tra u ma tic b ra in in ju ry (TBI) (iii) H o w ev er ,t h e hig hest ag e gr o u p incidence is b etw een 19 and 29 ye ar s, re p res en ti n g ap p ro xima tel y o n e-q u ar te ro fp at ie n tsw it hc ra n ia lt ra u m a (i v) C h il dr en (18 ye ar s an d yo u n ger) rep re se n ted almost 45% o f the p at ien ts w it h he ad in ju ry Ti er n ey et al .[ 4 1] The p u rp os e w as to det er mine w h et her gender diff er ences exist ed in h ea d-nec k se gm en t k inema ti c and neur o m us cu la r co n tr o lv ar ia b les re sp o n se s to an ext ern al fo rc e ap p lica tio n wi th an d w it ho u t ne ck m u sc le p re ac ti va tio n 20 fe m ale s 20 m ale s Ad u lt C o ho rt st ud y (i) G ender diff er ences exist ed in h ea d-nec k se gm en t d yna mic st ab il iza tio n d ur in g h ea d an gu la r accelera ti o n (ii) F emales exhib it ed significa n tl y gr ea ter he ad-nec k se gm en t p ea k an gu la r accelera ti o n an d d isp lacemen t th an males d esp it e ini ti at in g m us cl e ac ti vi ty ea rlier (SCM o n ly ) and usin g a gr ea te r p er cen ta ge o f th eir maxim u m h ea d-ne ck se gm en t m us cle ac tiv it y Tr el ea ve n et al .[ 31 ] This st u d y me asur ed asp ec ts o f cer vical m us cu losk elet al fu n ct ion in a group of p at ie n ts (12) wi th p o st co nc ussio n al he ad ache (PCH) and in a n o rma l co n tro lg roup 8m al es (15– 4 8 yo) 4 fema les (20– 4 4 yo ) Retr os p ecti ve st u d y (i) T w el ve o f the 15 elig ib le p at ien ts co n sen te d to en ter th e st u d y (ii) The most fr eq uen t ma jo r sym p to m at ic se gmen ts w er e C1 -C2, C2-C3, C0-C1, an d C 3-C4. Si gn s o f ce rv ic al ar ti cu lar an d m u sc u la r d ys fu n ct ion dist in guished the PCH gr o u p fr o m th e co n tr o lgr o u p (iii) A s u p p er cer vical jo in t d ysf unc tio n is a fe at ur e o f cer vicog enic ca us es o f he adac he ,t he re su lt s o f this st u d y supp o rt th e in clu si on of a p re ci se ph ys ic al exa mina tio n o f the cer vica lr eg io n in diff er en ti al dia gnosis o f p at ien ts suff er in g p er sist en t h ea dac h e fo llo w in g co n cu ssio n
Ta b le 2: C o n ti n u ed . A u th o rs/s ec tio n s St ud y o b jec ti ve P o p u la ti o n M et h o d s M ai n o u tco mes/findin gs Wa ta n ab e et al . [20] The sp ecific go als o f this re vie w inc lude (1) det er mina tio n o f eff ec ti ve in te rv en ti ons for P T H (2 ) d ev el o p m en t o f tr ea tm en t re co mmenda ti o n s (3) iden tifica tio n o f ga p s in the cu rr en t m edical li te ra tu re re ga rd in g P T H A tre at m en t (4) sug ge st io n s fo r fu tur e d ir ec ti ons in re se arc h to im p rove out com e for p er sons w it h P T H A Ad u lt Ch il d L it er atu re re vi ew The le ve lo f evidence: Amer ica n A cadem y o f N eu ro lo gy cri te ria (i )H ea dp ai nm ay b e re la te dt od ir ec td am ag et ot h e sk u ll or br ai n ti ssu e; m u sc u lar ,t en d in ou s, an d /or liga men to u s in jur y to the cer vi ca ls p ine; and in ju ri es to p er ip h era lner ves. O th er ner vo u s syst em in jur ies, suc h as vi su al an d ve st ibu la r sy ste m d am age, al so m ay co n tr ib u te to he ad ache sy ndr o mes (ii) B io logicall y bas ed in ter ve n tio n s inc luded a va ri ety of bi ofe ed b ac k m ec h an is ms ,p h ys ic al th er apy an d ma n u al th era p y, immo b iliza tio n d ev ices, ice ,a nd in jec tio n s We ig h tm an et al . [1 7] Th e p u rpo se o f th is art ic le is to p ro vide a summa ry o f the de ve lo p m en t p ro cess and to sha re sp ecific re co mmenda ti o n s fo r P T p rac tice w it h ser vice mem b ers w ho sust ai n MTBI Mi li ta ry and civ il ia n p opu la ti ons L it er atu re re vi ew MTBI-r ela ted , ev idence-bas ed re vie ws an d guidelines (i) D et er mine the dis ab ili ty an d its se ve ri ty re la te d to th e n ec k, ja w ,a n d h eadac h es (ii) Ph ysical th era p y in ter ve n tio n s wi th th e st ro n ge st ev idence in the tr ea tm en t o f P TH inc lude a m ul ti mo dal ap p roac h o f sp ecific tr ainin g in ex er cis e and p o st ural re tr ainin g ,st re tc hin g and er go no mic ed uca tio n, an d ma ni p u la ti o n an d/o r mo b iliza ti o n in co m b ina tio n w it h ex er cis e
Table 3: Most common symptoms of mTBI according to their categories [4, 6, 11–13].
References Cognitive Somatic physical Affective emotional Sleep disturbance
Marshall, 2012 [11] Hanson et al., 2014 [6] Hynes and Dickey, 2006 [12] Scorza et al., 2012 [13] McCrory et al., 2013 [4] (i) Confusion
(ii) Retrograde amnesia (iii) Anterograde amnesia (iv) Loss of consciousness (v) Disorientation (vi) Feeling foggy (in a fog) (vii) Vacant stare
(viii) Inability to focus (ix) Delayed verbal responses (x) Delayed motor responses (xi) Slurred
(xii) Incoherent speech (slurred) (xiii) Excessive drowsiness
(i) Headache (ii) Dizziness
(iii) Balance disruption (iv) Nausea
(v) Vomiting
(vi) Visual disturbances (vii) Phonophobia
(i) Emotional liability (ii) Irritability (iii) Fatigue (iv) Anxiety (v) Sadness
(i) Trouble falling asleep (ii) Decreased sleep (iii) Increased sleep
Hanson et al., 2014 [6]
(i) Feeling slowed down (ii) Difficulty concentrating (iii) Difficulty remembering (iv) Forgetting of recent information
(v) Confused about recent events (vi) Answers questions slowly (vii) Repeats questions
(i) Balance problems (ii) Visual problems (iii) Fatigue
(iv) Sensitivity to light (v) Sensitivity to noise (vi) Dazed
(vii) Stunned
(i) Nervousness (i) Drowsiness
Hynes and Dickey, 2006 [12]
(i) Dysphagia (ii) Seeing stars
(i) Deafness
(ii) Ringing in the ears (iii) Temporomandibular
Scorza et al., 2012 [13]
(i) Disorientation (ii) Stunned (iii) Vacant stare
(i) Blurred vision (ii) Convulsions (iii) Light-headedness (iv) Numbness (v) Tingling (vi) Tinnitus (i) Clinginess (ii) Depression (iii) Personality changes
Table 4: Summary table of the Whiplash-Associated Disorder (WAD) classifications and concussion symptoms that can manifest themselves in any grade of WAD [6, 20, 27, 28].
WAD classification Symptoms
0 No neck complaints
I Complaint of neck pain, stiffness, or
tenderness
II Neck complaint with
musculoskeletal signs
III Neck complaint, musculoskeletal
signs, and neurological signs
IV Fracture and/or dislocation
of the cervical region by a precise physical examination in differential diagnosis of 12 patients suffering of persistent postconcussion headache [31].
Following a whiplash, the cervical spine is often the source of a patient’s pain [4, 10]. The neck received the transmitted force of the impact and the same acceleration-deceleration mechanism that produces mTBI [28]. During the whiplash, the cause of cervicogenic and brain induced symptoms could be caused by either the mTBI or the cervical spine involvement or both at the same time [10]. There are
similarities between the symptoms of neck disorders and the symptoms of mTBI [19]. The most common posttraumatic symptom is headache [4]. Cervicogenic headache and post-traumatic headache are well-known conditions [4, 13, 19, 33]. In fact, those upper cervical impairments, if not diagnosed and treated, can lead to chronicity of postconcussion head-aches [10].
Cervicogenic headaches are common after a whiplash injury [16, 34]. Different studies showed that 3 to 4.6% of patients will develop chronic daily headaches after whiplash and 2% will be permanently disabled [34]. Upper cervical spine pain can arise from various anatomical structures such as muscles, joints, ligaments, and nerves [34]. Tensions in cervical muscles (trigger points) are the most common diag-nosed type of headache [16, 23]. Becker (2010) explained that headaches related to cervical spine disorders (CGH) remain one of the most controversial areas of headache medicine [34]. Dysfunctions of the craniocervical zygapophysial (C0 to C4) joints can also cause headaches [16, 30]. In patients with headaches following a whiplash injury, dysfunctions of the C2-C3 zygapophysial joint are highly prevalent, particularly if there is tenderness over the C2-C3 facet joint [34]. Cer-vicogenic headaches may be unilateral or bilateral with the dominance depending on one or more of the structures that are affected [16]. Pain location usually begins in the occipital
region of the neck [34]. After a whiplash injury, zygapophysial joints are clinically identified as the single most common source of pain in at least 50% of neck pain. Furthermore, facet joints appear to be the most common source of pain in the neck, with or without headache [34]. King et al. (2007) showed in their retrospective study, which included 173 patients, that manual examination had a high degree of sensitivity during zygapophysial joint pain evaluation [35]. Tension in the cervical muscles has the potential effect of reducing neck movement and generating local pain [16, 18]. A bad posture or sleeping position as well as physical activity performed with a faulty motor strategy can lead to neck pain and pain irradiating to the head [19]. In 2013, the Cervicogenic Headache International Study Group (CHISG) developed the diagnostic criteria for CGH [33] (see the following).
Summary of the Cervicogenic Headache (CGH) Diagnostic Criteria [33]
Unilaterality of pain, although it is recognized that bilateral cervicogenic headache may occur.
Restriction in range of motion in the neck.
Provocation of usual head pain by neck movement or sustained awkward neck positions.
Provocation of usual head pain with external pressure over the upper cervical or occipital region on the symptomatic side.
Ipsilateral neck, shoulder, or arm pain, usually of a vague nonradicular nature, occasionally radicular. Posttraumatic headaches are a serious contributor to disability following cranial, cerebral, and cervical injury. Therefore, evaluating the cervical region after a head trauma is recommended [4]. This recommendation will highly con-tribute to limiting morbidity of mTBI and, furthermore, to help clinicians identify the International Headache Society (IHS) cervicogenic characteristics on mTBI patients. One of the improvements of SCAT3 and Child-SCAT3 compared to the SCAT2 is the introduction of the cervical assessment in posttrauma evaluation [4]. Knowing that the mechanism of mTBI is an external force transmitting energy to the head, it is possible that the neck, supporting the head, can also be injured during such an external force [11, 12, 16]. The Zurich consensus for concussion in sports (2012) recommended a multidisciplinary approach for patients who suffer PCS symptoms, such as headaches lasting longer than 6 weeks [4]. 6.3. Treatments. The majority of articles in the literature cur-rently focus on the diagnosis of mTBI, but few are dedicated to its management and treatments [7]. The 2012 Zurich con-sensus on concussion in sport suggested physical and cogni-tive rest until the end of the acute symptoms after trauma and a multidisciplinary approach involving experienced health care professionals when treating mTBI [4]. In their retro-spective analysis, Moser et al. (2012) analyzed 49 high school and collegiate athletes (mean = 15.0 years old) and suggested
that a period of cognitive and physical rest may be a useful mean of treating concussion-related symptoms [21]. This recovery time allows for a period of 7 to 10 days before the athlete returns to competition [2]. During this period, the symptoms should be evaluated daily and all activities that increase these symptoms should be stopped [4]. A Cochrane study mentioned that, based on present literature, no acutely initiated intervention has been clearly associated with a positive outcome for patients who sustain mTBI [36].
Return-to-play is allowed when athletes are symptom-free at rest, are able to do a full practice with contact without symptoms, no longer take any medications, and have returned to their baseline levels of cognitive functioning and postural stability [6].
The evaluation of the cervical region has been included as a new part of the SCAT3/Child-SCAT3, and a full clearance is essential before return-to-play [4]. According to some authors, post-mTBI subjects must have no pain in the neck, full mobility, and an adequate bilateral general strength to restart their sporting activities [12].
Treatments such as vertebral manual therapy, cervical tractions, manipulations, and exercises can relieve neck pain [16]. Brolinson (2014) has demonstrated that interventions of spinal manual therapy, physiotherapy, and neuromo-tor/sensorimotor training are more effective for mTBI recov-ery compared to a program of rest and exercises [7]. Another study demonstrated that the physical status of individuals with neck pain is improved with an exercise program combin-ing manipulation, proprioceptive neuromuscular facilitation, acupressure on trigger points, and range of motion exercises, along with proprioceptive exercises compared to a neck pain control group of similar patients treated with information and advice [29]. Treatment of the cervical spine (sustained natural apophyseal glides) has been shown to be effective in 17 indi-viduals with suspected cervicogenic dizziness compared to a control group (17 adults) [37]. Schneider et al. (2014) estab-lished that a significantly higher proportion of post-mTBI individuals (more than 3 weeks after trauma) were medically cleared to return to sport within 8 weeks of initiating treat-ment if they were treated in physiotherapy with cervical spine and vestibular rehabilitation compared to a control group [10]. Another study recruited 128 mTBI adults with either PCS or cervicogenic/vestibular symptoms [27], who completed the 22-symptom postconcussion symptoms scale question-naire. Their results demonstrated that the questionnaire does not reliably discriminate between both types of patients. They concluded that clinicians should consider specific testing of exercise tolerance and perform a physical examination of the cervical spine and the vestibular/ocular systems to determine the etiology of postconcussion symptoms and to consider treating these accordingly [27]. Assessment and treatment of the cervical spine and vestibular system in the presence of persistent dizziness, neck pain, and/or headaches may facili-tate functional and symptomatic improvements and shorten recovery in post-mTBI subjects [7, 10].
There is little evidence in clinical trials on the treatment of PTH. A study by Bonk et al. (2000) has shown that physio-therapy treatments decrease pain and increase cervical range of motion compared to a control group in a cervical collar for
a period of 6 and 12 weeks after trauma [38]. The physiother-apy programs consisted of active and passive mobilizations, postural strengthening, the application of ice, and exercises that are efficient for PTH.
Regarding the cervical muscular system, several changes are observed following a trauma such as mTBI or whiplash. There is still nonempirical support that stronger neck muscles could reduce the risks of mTBI on the field [11, 39]. In fact, Mihalik et al. (2011) evaluated the effect of cervical strength on head impact in 37 hockey players (average 15 years old) and they concluded that the hypothesis of neck strength decreas-ing head acceleration was not supported [39]. Recent publica-tions identify the importance of neck musculature in the pre-vention of concussions. Two hypotheses are presently under debate in the literature. The potentially modifiable risk factors for concussion are neck strength and impact anticipation [40]. Tierney et al. (2005) demonstrated that males have a better head-neck segment dynamic stabilization than females when angular acceleration is sustained by the head in a study including 20 males and 20 females [41]. Furthermore, a descriptive study demonstrated that greater neck strength and anticipatory cervical muscle activation (bracing for impact) can reduce the magnitude of the head’s kinematic response in a population of 46 contact sport athletes (male and female) aged between 8 and 30 years [40]. Another study on a group of 49 football players (high school/collegiate) has shown that the odds of sustaining higher magnitude head impacts are reduced with better cervical strength and lower angular displacement following impact [42]. However, their findings did not show that stronger and larger neck muscles in players decreased head impact severity [42]. Meanwhile, Collins et al. (2014) concluded, in their study, which included 6704 high school athletes, that neck strength can be a valuable screening tool to prevent concussion [43]. Further research is needed to clarify these hypotheses and the actual role of neck strength in reducing risk of concussion.
A study by Leddy et al. (2012) for mTBI subjects slow to recover shows that a lightweight level of exercise can be beneficial [44]. Kozlowski et al. (2013) recently published a cross-sectional study about the exercise impact on 34 patients with PCS and a control group of 22 patients [3]. Conclusions showed that patients with PCS had a symptom-limited response to exercise, and the treadmill test was a potentially useful tool to monitor the recovery from PCS [3].
Other physiotherapy treatments, such as vestibular reha-bilitation, visual training, cardiovascular training, and the treatment of cervical dysfunctions, have shown some promis-ing avenues, but further studies are needed [4, 10, 14, 17, 20].
7. Conclusion
In conclusion, mTBI is a complex injury and needs to be taken care of by different medical specialists working together toward the same goal, recovery [4]. The evidence of cervical spine involvement in mTBI is becoming apparent, but there is a lack of sound evidence in the literature [25]. Our findings have implications for further research. The hypothesis of cervical spine involvement in post-mTBI symptoms and in PCS is supported by increasing evidence and largely accepted.
Health professionals should consider assessing the cervical spine of patients affected by mTBI. Some original data articles support this theory and show that persistent headache and postconcussion syndrome are often related to musculoskele-tal pathology of the cervical spine. For the mTBI management and treatment, few articles in the literature are available, but well-defined studies showed interesting results about manual therapy (cervical and vestibular) and exercises as effective tools for health care practitioners. Further studies are needed to establish an adequate evaluation and determine guidelines for treatments. The evaluation and treatment of the cervical region are a major step to improve mTBI rehabilitation.
Appendix
See Figure 1 and Tables 1, 2, 3, and 4, and also see “Summary of the Cervicogenic Headache (CGH) Diagnostic Criteria [33]” in Section 6.2.
Abbreviations
mTBI: Mild traumatic brain injury
ICL: Index to Chiropractic Literature
PEDro: SportDiscus, Physiotherapy Evidence Database
CINAHL: Cumulative Index to Nursing and Allied Health Literature
CDC: Centers for Disease Control and Prevention
TBI: Traumatic brain injury
PCS: Postconcussion syndrome
MRI: Magnetic Resonance Imaging
WAD: Whiplash-Associated Disorder
IHS: International Headache Society
PTH: Posttraumatic headache
CGH: Cervicogenic headache
GCS: Glasgow Coma Score
SAC: Standardized Assessment of Concussion
BESS: Balance Error Scoring System.
Competing Interests
The authors declare that they have no competing interests.
References
[1] C. Tator, G. Bray, and D. Morin, “The CBANCH report—the burden of neurological diseases, disorders, and injuries in Canada,” The Canadian Journal of Neurological Sciences, vol. 34, no. 3, pp. 268–269, 2007.
[2] M. R. Borich, K. L. Cheung, P. Jones et al., “Concussion: current concepts in diagnosis and management,” Journal of Neurologic
Physical Therapy, vol. 37, no. 3, pp. 133–139, 2013.
[3] K. F. Kozlowski, J. Graham, J. J. Leddy, L. Devinney-Boymel, and B. S. Willer, “Exercise intolerance in individuals with postcon-cussion syndrome,” Journal of Athletic Training, vol. 48, no. 5, pp. 627–635, 2013.
[4] P. McCrory, W. H. Meeuwisse, M. Aubry et al., “Consensus state-ment on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012,” British
![Table 3: Most common symptoms of mTBI according to their categories [4, 6, 11–13].](https://thumb-eu.123doks.com/thumbv2/123doknet/14606362.731803/16.900.78.830.128.641/table-common-symptoms-mtbi-according-categories.webp)