Prenatal Ultrasound Screening: False Positive Soft Markers May Alter Maternal Representations and Mother-Infant Interaction
9
0
0
Texte intégral
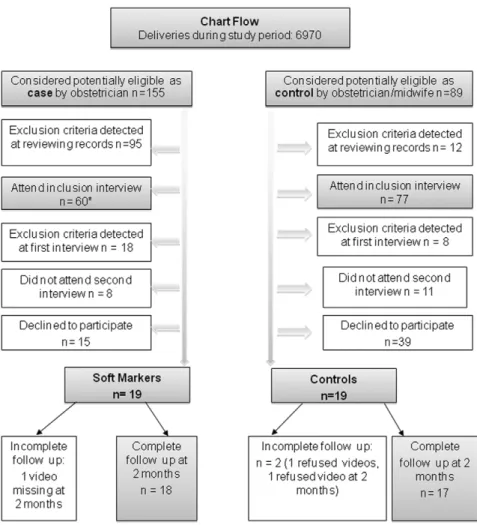
Figure

Documents relatifs