Decentralization and Health Service Delivery:Uganda Case Study by
Alfred Boateng Poku
B.A. Hons. Geography and Resource Development University of Ghana, Legon, Ghana, 1993
Submitted to the Department of Urban Studies and Planning in Partial Fulfillment of the Requirements for the Degree of
Master in City Planning at the
Massachusetts Institute of Technology February 1998
@ 1998 Alfred B. Poku All rights reserved
The author hereby grants to MIT permission to reproduce and to distribute publicly paper and electronic
copies of this document in whole or in part.
Signature of Author:
Department of Urban Studies and Planning February 5,1998 Certified by:
Paul J. Smoke Associate Professor of Political Economy and Planning iesis Supervisor Accepted by:
Lawrence Bacow Professor of Law and Environmental Policy Chairman, Master in City Planning Committee
DECENTRALIZATION AND HEALTH SERVICE DELIVERY:UGANDA CASE STUDY
By
ALFRED B. POKU
Submitted to the Department of Urban Studies and Planning on February 5, 1998 in Partial Fulfillment of the
Requirements for the Degree of Master in City Planning
ABSTRACT
Uganda has embarked on public sector reforms for the past decade. One of the most notable is the decentralization policy, which seeks to devolve powers from the central government to the local governments. Local governments have been given financial, administrative, planning and implementation responsibilities; they have been empowered to deliver services to their respective communities. The rationale for decentralization is that it is said to promote a more responsive and equitable service delivery; decision-makers are closer to the people and thus the community can demand services they need. One of the decentralized services that has received recent attention is health. This study focuses on the role of local governments in preventive health service delivery. I assessed the successful performance of Nama sub-county in Mukono in the context of decentralization policy. The study revealed remarkable improvements in vaccination rates. Successful implementation of the immunization program resulted from the role of the sub-county health committees in making health-related information
available; data on demographics and prevalence of diseases compiled by the health unit have provided the district with a guide to a more effective intervention. The findings also show that control, support and supervision from higher levels played a major role in effective preventive health service delivery. Finally, success was accomplished through extensive community mobilization, and a high degree of flexibility and coordination in the use of alternative service providers.
Thesis Supervisor: Paul Smoke
ACKNOWLEDGMENTS
I am very grateful to the Department of Urban Studies and Planning (MIT) and the United Nations Development Program for financial support for the research. Special thanks go to Professor Paul Smoke and James Morrison for the valuable contribution they made. Their constructive suggestions helped me to critically reassess my thinking and
analyze issues that I encountered.
The accomplishment of this work would not have been possible without the support from Mukono District Administration. I would like to thank Dr. E.K. Tumushabe (District Medical Officer, Mukono, Uganda), Mr. Sam Kisense (Chief Administrative Officer, Mukono,Uganda), Tamale Issa (Medical Assistant, Katoogo Health Unit, Mukono,Uganda).
I extend my sincere gratitude to Mr. Haruna Kyamanya (Assistant Resident Representative,United Nations Development Program,Uganda), Mr. John Leonard
Rucogoza and Mr. Obong (Directors of Local Administration, Ministry of Local Government, Uganda). Finally, my profound gratitude goes to Harriet Birungi, Patrick Madaya and Susan Mirembe (Makerere Institute of Social Research,Uganda) for their support in data collection.
CONTENTS
CHAPTER N ...
7
1.1 IN T R O D U C T IO N ... 7
1.2 B A C K G R O U N D ... 7
1.3 RESEARCH PROBLEM ... 9
1.4 OBJECTIVES OF THE STUDY ... 12
1.5 RESEARCH
QUESTIONS
... 121.6 M ETH O D O L O G Y ... 13
CHAPTER TWO...
15
2.1 DECENTRALIZATION POLICY AND INSTITUTIONAL CHANGES... 15
2.2 INSTITUTIONAL CHANGES IN THE HEALTH SECTOR... 17
2 .3 F U N D IN G ... 19
CHAPTER
...
23
3.1 A SUCCESS CASE . .. ... . ... ... ... 23
3.2 FACTORS THAT EXPLAIN THE SUCCESS ... 24
CHAPTER FOUR ...
40
4.1 CONCLUSIONS...40
4.2 RECOMMENDATIONS... 45
LIST OF TABLES
TABLE 1: ALLOCATION OF RECURRENT AND DEVELOPMENT EXPENDITURE
EXPRESSED AS A PERCENTAGE OF CENTRAL GOVERNMENT'S BUDGET...8
TABLE 2:COMPARISON- INFANT MORTALITY RATES ... 10
TABLE 3: LITERACY RATE AMONG WOMEN... 11
TABLE 4: PERCENTAGE OF POPULATION WITHIN 5KM OF A HEALTH UNIT 11 TABLE 5: SIGNIFICANT IMPROVEMENT IN IMMUNIZATION RATE: ... 24
TABLE 6: KATOOGO: 1995/96 HEALTH SURVEILLANCE FOR PREVENTIVE C A R E ... 2 6 TABLE 7: KATOOGO: 1995/96 HEALTH SURVEILLANCE FOR PREVENTIVE C A R E ... 2 6 TABLE 8: BURDEN OF DISEASE AND ALLOCATION OF FUNDS ... 29
TABLE 9:1995/96 FY SUPPORT PROGRAMS ... 31
TABLE 10: 1996/97 FY SUPPORT PROGRAMS... 31
TABLE 11: 1995/96 FY MOBILIZATION ACTIVITIES... 34
TABLE 12: 1996/97 FY MOBILIZATION ACTIVITIES... 34
TABLE 13: TRADITIONAL BIRTH ATTENDANT REPORT ... 37
TABLE 14: SELECTED SUPPORT RECEIVED BY TBAS - 1995/96 FY ... 38
LIST OF FIGURES
FIGURE 1: DECENTRALIZED HEALTH ADMINISTRATIVE SYSTEM... 21FIGURE 2:CHANGES IN FINANCIAL FLOWS TO HEALTH SERVICES... 22
GLOSSARY OF TERMS
DHC DISTRICT HEALTH COMMITTEE
DHMT DISTRICT HEALTH MANAGEMENT TEAM
DHSP DISTRICT HEALTH SERVICES PROJECT
DMO DISTRICT MEDICAL OFFICER
HA HEALTH ASSISTANT
HUMC HEALTH UNIT MANAGEMENT COMMITTEE
LC LOCAL COUNCIL
MFEP MINISTRY OF FINANCE AND ECONOMIC PLANNING
MOLG MINISTRY OF LOCAL GOVERNMENT
NGO NON-GOVERNMENTAL ORGANIZATION
NMS NATIONAL MEDICAL STORES
SCHC SUB-COUNTY HEALTH COMMITTEE
VHC VILLAGE HEALTH COMMITTEE
CHAPTER ONE
1.1 INTRODUCTION
For the past ten years, the government of Uganda has embarked on a number of reforms geared towards enhancing the capacity of the public sector to deliver more efficient and responsive services to the wider population. One of the reforms being undertaken is decentralization; this is a policy aimed at transferring power to the local governments to provide services in their respective jurisdictions. Decentralized health
service delivery has evolved as a way to expand services to the remote places where the infant mortality rate remains relatively high at 112 (United Nations 1994). Preventive
health interventions, such as immunization, have been pursued to reduce the infant mortality rate; however, lack of appropriate institutional forms, poor knowledge of the remote villages and weak community mobilization have undermined the performance of both local and central governments in achieving their targets. If effective interventions are not sought, infant deaths could continue to rise. This paper examines a remarkable performance of one district where immunization targets have been achieved. The focus of this paper is on the strategies adopted by newly formed local health committees to
improve their vaccination programs.
1.2 BACKGROUND
The economic history of the country has been marked by social, economic and political instability. During the period between 1961 and 1970, Uganda had an annual economic growth rate of 5.1%; however, in the period between 1970 and 1980, the country experienced a decline in GDP of about 25% ( Jitta et al., 1996). This economic 7
deterioration had adverse impacts on the health sector. Recurrent and development
budgetary allocations to the health sector have continued to decline. Please see table 1 for the decline in financial flows for health services as a percentage of the central
government budget.
TABLE 1: ALLOCATION OF RECURRENT AND DEVELOPMENT EXPENDITURE EXPRESSED AS A PERCENTAGE OF CENTRAL GOVERNMENT'S BUDGET
YEARS 1982/83 1983/84 1984/85 1985/86
RECURRENT 5.59 4.47 3.72 2.14
DEVELOPMENT 5.59 1.76 3.73 0.82
SOURCE: 1982/83-87/88 BACKGROUND TO THE BUDGET, GOVERNMENT OF UGANDA
Owing to the decreasing allocation of funds, the health sector faced problems ranging from technical inefficiency to ineffective and unresponsive utilization of resources. In addition, the health system has remained oriented to curative services, but the major causes of morbidity and mortality are preventable. Nutritional status among
children is very low, and service deficiencies have accounted partially for the high infant mortality rate. Also, expenditure on health is lower than what is required to provide preventive health services. Per capita expenditure is US $ 7.60 while the recommended expenditure is $12 (Jitta et al.,1996). This situation has resulted in poor services to the population, especially those in rural areas.
Policy-makers have been seeking alternative ways to provide services that are responsive to communities, especially at the local level. In 1986, when the National Resistance Movement took power, a number of reforms were pursued to mitigate some of
the problems in the health sector, partially through the government's broader decentralization policy.
Current thinking in health service management has focused on decentralization as one of the ways to address existing inefficiencies and make services more responsive to
local preferences. Decentralization is said to be appropriate in health service delivery because of the spatial variation in patient preferences and the ability of local officials to
identify needs better. " Decentralized management is in a better position to deliver such services. Decentralized management can be more flexible and adaptable; managers are closer to the sphere of influence produced by patients and the health care personnel providing their service" (Boissoneau, 1986). Contemporary literature also posits that decentralization creates a better environment for initiative. It is claimed that
decentralization improves health service management. The extent to which decentralized health service delivery results in better services, however, has yet to be explored.
1.3 RESEARCH PROBLEM
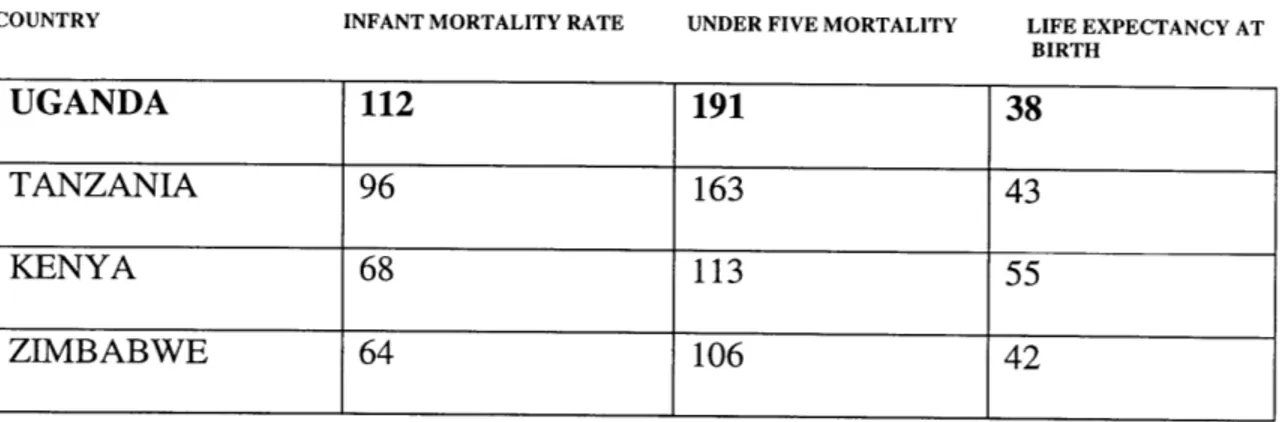
The provision of health services is a complex one in the sense that many variables affect the health of individuals and communities. Uganda's health sector has been plagued with serious problems, such as inadequate drug supply, mismanagement of the health units, and inaccessibility. Centralized health institutional structures have not responded well in providing services to the people; preventive and promotive health interventions have failed to achieve the desired results. Thus, infant mortality rates in Uganda are still higher than in the neighboring countries. In 1994, the infant mortality rate was 112 per
addition, the under-five mortality rate is as high as 203 per 1000 live births ( United States Bureau of Census, 1994). In the central region of the country (location of the study area), 11 newborns out of 12 survive infancy (Jitta et al., 1996).
Table 2:COMPARISON- INFANT MORTALITY RATES
COUNTRY INFANT MORTALITY RATE UNDER FIVE MORTALITY LIFE EXPECTANCY AT
BIRTH
UGANDA 112 191 38
TANZANIA 96 163 43
KENYA 68 113 55
ZIMBABWE 64 106 42
SOURCE: 1. DEPARTMENT OF INTERNATIONAL ECONOMIC AND SOCIAL AFFAIRS. UNITED NATIONS. WORLD POPULATION PROSPECTS 1994. NEW YORK. UN 1994.
2. UNITED STATES BUREAU OF THE CENSUS (BUCEN). INTERNATIONAL DATA BASE VERSION DATED MARCH,1994.
In all categories shown in Table 2, Uganda is worse than all the other countries in the region. These health indicators call for more attention to preventive services.
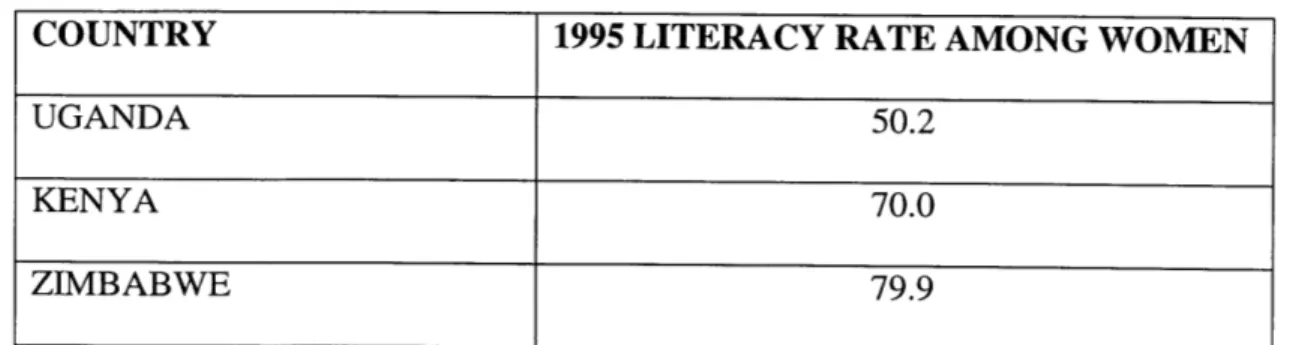
Moreover, dissemination of information about immunization programs is poor. Women do not often know when to take their children for immunization; high illiteracy has been one of the major problems. Table 3 shows that Uganda's literacy rate among women is relatively low compared with a number of neighboring countries. This tends to affect the extent to which information on vaccination cards can be read and understood.
Table 3: LITERACY RATE AMONG WOMEN
COUNTRY 1995 LITERACY RATE AMONG WOMEN
UGANDA 50.2
KENYA 70.0
ZIMBABWE 79.9
SOURCE:1. WORLD HEALTH ORGANIZATION. HEALTH FOR ALL GLOBAL INDICATORS. SEPTEMBER, 1996.
2. UNITED NATIONS EDUCATIONAL, SCIENTIFIC AND CULTURAL ORGANIZATION. HEALTH STATISTICS
1995.
These problems have been compounded by poor accessibility to health units. Most of the health centers are located in urban areas. In 1992, only 49% of the Ugandan population lived within 5 kilometers of a health center and had access to essential drug
kits. Table 4 shows the distribution of the population in different regions living within 5
kilometers of a health unit.
Table 4: PERCENTAGE OF POPULATIONWTI (MOAHATH TTNT
SOURCE: THE THREE YEAR HEALTH PLAN FRAME. GOVERNMENT OF UGANDA1993/94 -1995/96.
The problems in the health sector have prompted the search for more effective ways to improve accessibility of health services in rural Uganda. While preventive care is an obvious approach to control and prevent diseases, the appropriate institutional form of service delivery is not immediately clear. An elaboration of alternative planning and
REGION PERCENTAGE OF POPULATION
CENTRAL 56
EASTERN 60
NORTHERN 27
WESTERN 47
implementation mechanisms will illuminate some lessons for policy-makers and
communities regarding the provision of preventive services. Against this background, it is imperative to assess the role of local governments in preventive health programs as it is evolving under the ongoing decentralization policy.
1.4 OBJECTIVES OF THE STUDY
The main focus of the study is to see if, why, and how the new decentralized institutional arrangements for health care have responded better to the needs of
beneficiaries. I assess the effectiveness of the mechanism used by local governments to target and provide services. Moreover, the study is geared towards identification of factors that promote or inhibit health service delivery. The findings can serve as a framework for policy makers and health service providers in their pursuit of more effective service delivery.
1.5 RESEARCH
QUESTIONS
In order to evaluate the implications of these changes, I examine the following questions.
1) Do newly created decentralized structures help improve health service delivery at the sub-county levels? In what ways?
2) Are the decentralized health programs responsive to local preferences, taking into account the burden of disease (BOD) in the community under study? If so, in what ways? 3) Are higher-level control measures necessary for decentralized local health service delivery? If so, what kinds?
4) Do community and service provider collaboration have the potential for effective health service delivery? If so, which mechanisms seem most promising?
5) Can potential alternative actors (independent service providers) be incorporated into the process without undermining their autonomy? If so, in what ways?
1.6 METHODOLOGY
The role of the sub-county governments (LC 3) in health service delivery is the main focus of the research, although some selected cases at the district level (LC 5, a higher level) were analyzed. The reason for studying the sub-counties was that substantial financial autonomy was given to them in 1993, so that they retain 65% of all revenues raised in their respective jurisdictions. In addition, they have significant responsibility for preventive health care.
Semi-structured interviews were conducted with key informants: local leaders, sub-county chiefs, local council chairmen, heath unit personnel, sub-county medical officers, district medical officers and members of district health management teams. Questions were asked about the new institutional changes, the new roles defined, and how they affected performance. Health workers were interviewed regarding how they implemented the preventive health programs, what conditions existed for better performance, and why they could not do this before decentralization. Selected
beneficiaries from the community were interviewed on how they responded to programs, what they see as changes and how they perceive the changes in implementation as effective. Focus group discussions were also held with personnel from the district population and planning office.
Finally, secondary sources were reviewed. Among the health data analyzed are the district progress reports, health unit annual reports, minutes of meetings, national, district and sub-county budgets.
CHAPTER TWO
2.1 DECENTRALIZATION POLICY AND INSTITUTIONAL CHANGES Decentralization policy was initially introduced in 1987 when the National Resistance Movement enacted the Resistance Councils (RC)/Committees Statute. The policy aims at transferring central government functions and powers to the local
governments. It seeks to give certain responsibilities to the lower government council "in order that decisions are made as close as possible to where services are delivered." The statute defined the autonomy of the local councils to carry out functions in their
respective jurisdictions. However, this policy existed only on paper and local authorities were never able to exercise any kind of autonomy: "By 1990, it had become evident that the application of the 1987 RC Statute had only succeeded in raising political
consciousness and promoting deconcentrated field administration, but had failed to effectively empower the people and to promote democratic local
self-governance."(Okuanza and Lubanga 1995). Planning, problem identification,
implementation and resource allocation were primarily central government functions. It was not until 1993 that the local councils began to enjoy substantial autonomy.
In December 1993, the government released the New Local Government Statute to reinforce the dormant 1987 Resistance Councils Statute. The 1993 Local Governments (Resistance Councils) Statute consolidated the Resistance Councils. The Resistance Councils system is made up of five tiers consisting of the following:
2) County Resistance Councils - LC 4 3) Sub-County Resistance Councils - LC 3
4) Parish Resistance Councils - LC 2
5) Village Resistance Councils -LC 1
Among the functions that were vested in the lower local councils are identifying problems, formulating and reviewing development plans, making plans for infrastructure development, and providing municipal works and services (Uganda Local Government Statute, 1993). In essence, authority over administration, planning, politics and finances was devolved from the center to the districts and the lower Resistance Councils.
Moreover, the enactment of the 1993 Local Government Statute gave substantial autonomy to the districts in the areas of service provision. The sub-county governments were given revenue-raising responsibility; 50% (Uganda Local Government Act, 1993) and subsequently 65% of all revenues raised are to be retained at the sub-county level
(Uganda Local Government Act, 1997).
The decentralized institutions were further given legal backing through the provisions of the 1995 Constitution of the Republic of Uganda. Article 176 of the Constitution stipulates the local government status as the following:
The following principles shall apply to the local government system: 1) The system shall be such as to ensure that functions, powers and
responsibilities are devolved and transferred from the Government to the local government units in a co-ordinated manner;
2) There shall be established for each local government unit a sound financial base with reliable sources of revenue;
3) Appropriate measures shall be taken to enable local government units to plan, initiate and execute policies in respect of all matters affecting the people within
their jurisdiction;
4) Persons in the service of local government shall be employed by the local governments;
5) The local governments shall oversee the performance of persons employed by the government to provide services in their areas and to monitor the provision of government services or the implementation of the projects in their areas.
2.2 INSTITUTIONAL CHANGES IN THE HEALTH SECTOR
The decentralization reform as it relates to the health sector is geared towards the creation of unified health service provision at the district level. To achieve this objective, the central government's role in health service delivery was redefined. The central
government actors are the Ministry of Health and the Ministry of Local Government. The New Local Government Statute of 1993 coincided with the Ministry of Health's release of the White Paper on Health Policy.1 Since 1993, the health sector has undergone
institutional changes as a result of this decentralization policy. The key changes at each level are the following:
National Level
The Ministry of Health and Ministry of Local Government have been made responsible for coordinating and monitoring all the health projects in the districts. They also formulate health policies and serve as technical advisors.
1 The 1993 Local government statute differs from the MOH White Paper in one key area. In the Local Government Statute, the central government was responsible for the day -to -day administration of the hospitals, while the MOH White Paper gave that responsibility to the districts. At present, there is still no clear -cut distinction between the functions of the central government and the districts in hospital
administration.
District Level -LC 5
Before decentralization, the Ministry of Health and the Ministry of Local Government were responsible for health services administration. With decentralization, functions have been devolved to the district medical office and the sub-county
governments. The Local Governments Act of 1997 reiterated the functions of the districts in health service delivery. Districts are now responsible for the health centers,
dispensaries, sub-dispensaries, first aid posts, control of communicable diseases and the provision of primary health care services (Uganda Local Government Act 1997a) The functions include identifying health problems, setting priorities, and implementing projects.
New health committees have also been created. At the district level there is a district health management team, a coalition of health professionals including the district drug inspector, district nursing officer, district health educator, district health visitor, district ophthalmology clinical officer and the district vector control officer. Their main functions are to implement health programs in the district. Also, district health
committees have been established to coordinate health policies and the activities of Non-Governmental Organizations (NGOs) and other service providers in the district.
Sub-County Level - LC 3
Sub-county health committees have been established under the sub-county administrative structure. The functions of this committee are to make budget allocations for health services and to guide project implementation. This committee is composed of
nine members: one medical assistant and eight councilors who are elected by the council. Health unit management committees (HUMC) have been formed. They are composed of nine elected members from the community. They are responsible for the collection and utilization of user fees at the respective health units. The Health unit management committee also streamlines the performance of the health personnel; they make sure that they report to work on time and attend to patients promptly.
Village Level -LC 1
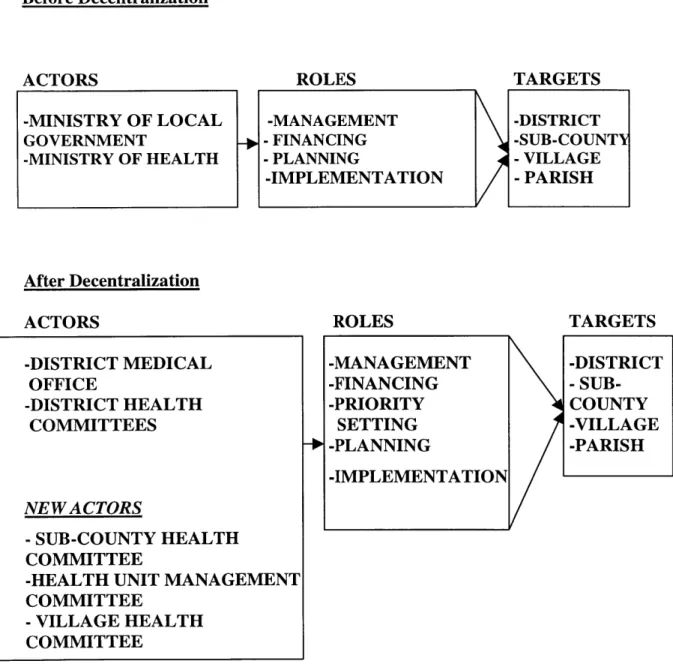
At the village level, village health committees have been set up to identify and report health problems to the health units. They comprise of the community health workers and their composition differs from village to village but they are often made up of three to seven elected members. Please see figure 1 (p.21) for a diagram of the structure of health service administration.
2.3 FUNDING
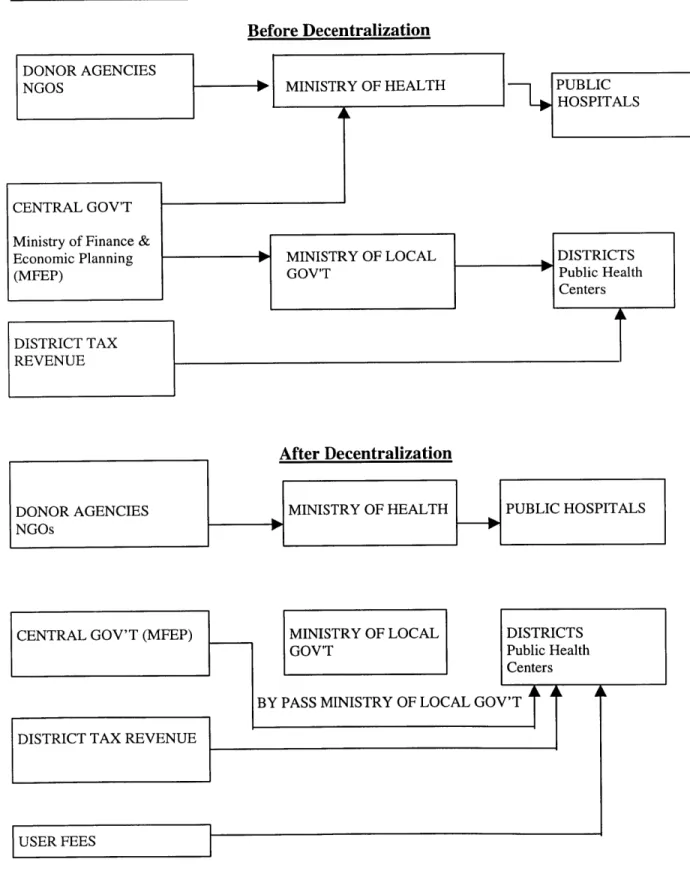
In Uganda, most of the health funding comes from donor agencies. During the 1990/91 financial year, the central government contributed 32% to public health while 60% came from external organizations (Jitta et al.,1996). Several changes occurred in the flow of funds after decentralization. Funds from the central government and donors are sent directly to the districts and thus districts receive delegated funds for recurrent budgets. The Ministry of Local Government no longer makes budget allocations for the districts, which now make their own decisions on health expenditure. Moreover,
decentralization has made more funds available; user fees have been introduced at most of the health units. The introduction of the user fee reform was geared towards improving health services. It is a way of making more funds available for purchases of medical supplies. These additional supplies made available are necessary to keep the health units running. In some areas, user fees have been important while in others they make no significant contribution. "In one district hospital (Mukono) health workers were able to receive allowances from user charge revenue at least two times a month in addition to their official salaries. This raised their morale and attracted more staff to work in that same hospital." (Jitta et al.,1996). Please see figure 2 (p.22) for the changes in financial flows to health services.
FIGURE 1
Before Decentralization ROLES -MANAGEMENT -FINANCING -PLANNING -IMPLEMENTATION TARGETS -DISTRICT -SUB-COUNTY - VILLAGE -PARISH After Decentralization ACTORS -DISTRICT MEDICAL OFFICE -DISTRICT HEALTH COMMITTEES NEW ACTORS - SUB-COUNTY HEALTH COMMITTEE-HEALTH UNIT MANAGEMENT COMMITTEE - VILLAGE HEALTH COMMITTEE ROLES -MANAGEMENT -FINANCING -PRIORITY SETTING -PLANNING -IMPLEMENTATION TARGETS -DISTRICT - SUB-COUNTY -VILLAGE -PARISH ACTORS -MINISTRY OF LOCAL GOVERNMENT -MINISTRY OF HEALTH
Figure 2: CHANGES IN FINANCIAL FLOWS TO HEALTH SERVICES Before Decentralization
DONOR AGENCIES
NGOS
--
.
[
MINISTRY OF HEALTH PUBLICHOSPITALS DISTRICTS Public Health Centers MINISTRY OF LOCAL GOV'T After Decentralization CENTRAL GOV'T
Ministry of Finance & Economic Planning
(MFEP)
DISTRICT TAX
CHAPTER THREE
3.1 A SUCCESS CASE
Mukono was selected as a study area because it was among the first 13 districts that were decentralized in the 1993/94 financial year, and thus an evaluation of it is more appropriate than an evaluation of districts that were decentralized later. Mukono's health plan implementation rate has also been better than other districts I examined, and it has a history of good performance in service delivery. This case is an exceptional one.
THE STUDY AREA-MUKONO DISTRICT
The district is located in southeastern Uganda and has a population of 965,800 people (1996 projections) and population density of 179/sq. km. Urban residents of the population constitute 11.92%. It consists of six counties, which are subdivided into thirty-two sub-counties. The key health indicators are an infant mortality rate of 102 per 1000 live births and a crude death rate of 22 per 1000 lives. There are 56 health units
distributed throughout the district. In all, there are 20 medical officers, 74 midwives, and 91 nurses.
Nama sub-county was the focus of the study and specific reference has been made to its health unit located in Katoogo. This is because of the strong role of Katoogo health unit workers in preventive care services.
Nama Sub-County: Katoogo Health Unit.2
SOURCE: HEALTH MANAGEMENT INFORMATION SYSTEM 107. DISTRICT MEDICAL OFFICE, MUKONO, 1996
3.2 FACTORS THAT EXPLAIN THE SUCCESS
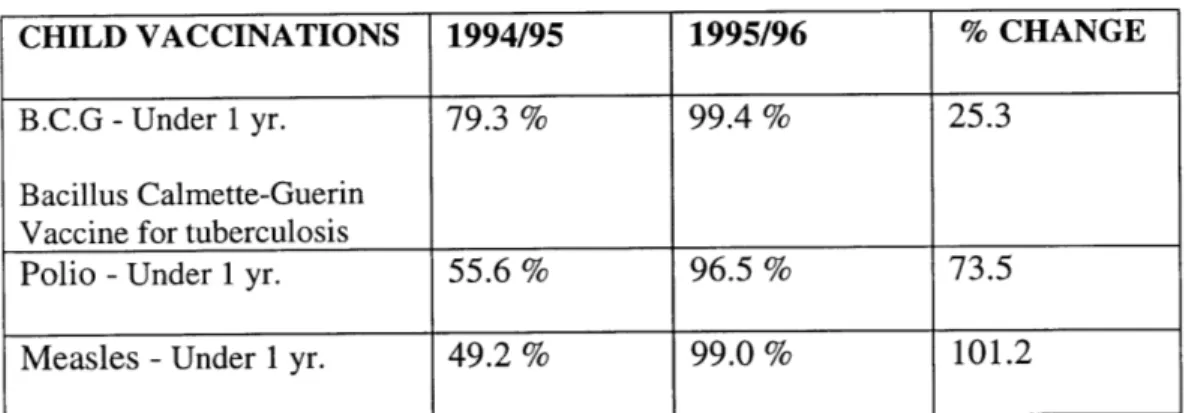
As shown in the above table, the sub-county has been able to achieve a remarkable performance in raising the vaccination rate. Some of the factors that contributed to this
success include the mechanisms used to identify problems, control and support from higher levels, community mobilization, and flexibility in the use of alternative partners for service provision.
2 The health unit has a Medical Assistant, an Enrolled Nurse, two Enrolled midwives, three Nursing Aids, a
Dresser and three other support staff, i.e., Porters. This makes a total of eleven personnel. This health unit serves a population of about 3,649 people.
CHILD VACCINATIONS 1994/95 1995/96 % CHANGE
B.C.G -Under 1 yr. 79.3 % 99.4 % 25.3
Bacillus Calmette-Guerin Vaccine for tuberculosis
Polio - Under 1 yr. 55.6% 96.5% 73.5
Measles - Under 1 yr. 49.2 % 99.0 % 101.2
An in-depth look at the most recent district and sub-county health plan review shows a tremendous increase in the rate of immunization after decentralization, as can be seen in table 5. This improvement in the immunization rates was better than that of other sub-counties I examined. Having identified this improvement, I proceeded to find out why and how success was accomplished.
1. Identifying problems
The village health committee serves as the main health needs identification unit after decentralization. Health related information on households is collected by the
committee. The health committee consults heads of households and community leaders to identify community problems. They compile and review the information and submit a draft report to the sub-county health committee (SCHC).
The sub-county health committees invites members of the community and the health unit management committee to identify priority areas. In consultation with the
health unit management committee and community health workers, the SCHC prioritize health interventions. Problem identification is performed in line with the national program priority areas, but community preferences prevail in most cases. The data collected by the village health committees have been very instrumental in the prioritization.
Please see Tables 6 and 7 for some of the vital health-related information collected and submitted to the district. The information in the tables is aggregate data collected from the community and compiled by the medical assistant in charge of the health unit, but more
disaggregate data on vulnerable children and those infected with diseases at specific areas are recorded. The information helps the medical assistants to identify areas that show some trends of serious disease incidence or epidemics; the pattern of disease is determined by assessing the number and types of cases reported to the health unit. Before decentralization, there were no such data collected and compiled for making informed decisions about local interventions.
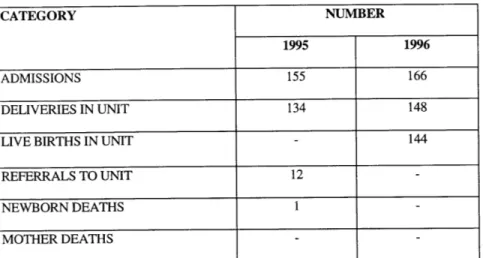
Table 6: Katoogo:1995/96 Health Surveillance for Preventive Care MATERNITY CATEGORY NUMBER 1995 1996 ADMISSIONS 155 166 DELIVERIES IN UNIT 134 148
LIVE BIRTHS IN UNIT - 144
REFERRALS TO UNIT 12
-NEWBORN DEATHS 1
MOTHER DEATHS
SOURCE: HEALTH MANAGEMENT INFORMATION SYSTEM 10 ANNUALKRPORT: U I I-IN I DEPARTMENT/MATERNAL CHILD HEALTH KATOOGO 1995/96
Table 7: Katoogo:1995/96 Health Surveillance for Preventive Care
CHILD HEALTH
CATEGORY NUMBER
1995 1996
NEW CHILDREN < 1 YEAR 533 488
NEW CHILDREN > 1 YEAR 101 34
WEIGHT < 75% WA 77 39
MALARIA 0-4 YEARS 1987 1574
SKIN DISEASES 0-4 YEARS 196 171
EYE INFECTIONS 0-4 YEARS 45 118
EAR INFECTIONS 0-4 YEARS - 43
ANEMIA 0 - 4 YEARS 91 86
TOTAL WEIGHED 533 45
SOURCE: HEALTH MANAGEMENT INFORMATION SYSTEM 107 ANNUAL REPORT: OUT PATIENT DEPARTMENT/MATERNAL CHILD HEALTH KATOOGO 1995/96
Tables 6 and 7 portray some of the vital information collected regarding maternal and child health. The recorded number of deliveries provides the medical assistant with accurate
information for immunization programs; the records are cross-checked to make sure all recently born children are vaccinated. Data on specific childhood diseases also help to identify major health problems.
On the basis of collected information which provides an improved understanding of health needs, sub-county health plans are made. The health plan is submitted to the district and integrated into the district heath plan. This integration of the sub-county plans into the district plan is an innovation developed by Mukono district and is now being tried in other districts. Please see figure 3 (p.28) for a summary of the integrated health planning process.
The integrated approach to health planning has the advantage of providing reliable data about specific areas to be targeted, and thus facilitates appropriate and cost-effective interventions. The specifics of the problem and the area suggest appropriate techniques for local conditions. Thus, service delivery can be modified to adapt to changes when the need arises. Integrated planning also minimizes implementation overlaps. " To avoid duplication of services and thus maximise resource utilization, Mukono District Health Team (DHT) has continued to encourage joint planning." (Mukono Health Plan 1995/96).
Figure 3: INTEGRATED HEALTH PLANNING -MUKONO DISTRICT
HEALTH UNIT COMMITTEES TRADITIONAL BIRTH
ATTENDANTS
SUB- COUNTY HEALTH PLAN
PROGRAM SCRUTINY BY DISTRICT HEALTH COMMITTEES
NGOS DISTRICT HEALTH MANAGEMENT TEAM
District Medical Officer District Health Inspector District Health Visitor District Health Educator.
DISTRICT HEALTH PLAN
The health data are used by the district to develop a specific strategy for resource allocation. The district uses the information to estimate the "burden of disease" (BOD). The burden of disease is calculated as a percentage of total life years lost, by ranking the number of cases with respect to the number of deaths they cause as well as the frequency of their incidence. Table 8 shows the burden of disease and the allocation of funds for 1996/97 FY. Although table 8 does not indicate a consistent positive relationship between the burden of disease and the allocation of funds, the burden of disease does provide the health officers with a better sense of health conditions. The burden of disease strategy, which was developed
after decentralization, is used in combination with other factors to make allocations. Again, I emphasize that this is a new approach in which some of the key data used in making
decisions are provided by the local health unit committees. Without this detailed information, district health administrators would be much more likely to either overestimate or
underestimate health problems.
Table 8: BURDEN OF DISEASE AND ALLOCATION OF FUNDS
DISEASE BOD AMOUNT ALLOCATED
IN THOUSANDS OF UGANDA SHILLINGS MALARIA 16.4 69,982 PERINATAL 15.1 188,709 NUTRITION DISORDERS 3.4 26,600 AIDS/STI 11.3 182,000 DIARRHEA DISEASES -TUBERCULOSIS 3.7 77,236
2. Control and Support
Since decentralization, supervision, guidance and control measures have increased in this district with respect to health services. The control and support of the sub-county come from
the district in four ways. The first one is support given by the district health teams in the form of provision of medical supplies, equipment and sensitization programs. Medical supplies are given to the to the sub-county during immunization days; they include vaccines and storage facilities. The provision of medical supplies and equipment to the sub-county health workers gives them some kind of confidence in implementing their health programs. The supplies are accounted for by the health unit medical assistant. The medical assistant always makes sure the equipment used for immunization is in good condition; otherwise the sub-county will be
denied support in the subsequent programs.
The district also supports sensitization programs in the sub-county. For example, during the FY 1995/96, from January through March, the district carried out a sensitization program of 60 community leaders as part of an immunization campaign. Also, during FY 1996/97,
163 parish leaders were sensitized about immunization (Mukono Health Plan Progress Report 1997). The sensitization program is a training program for the leaders. It covers the
strategies on how to get the community to bring their children in for immunization. Parish leaders are also educated on how to motivate and mobilize their people.
Tables 9 and 10 show some of the activities of support and supervision designed to build capacities at the lower levels of health administration. The district is committed to providing the necessary inputs for the program. The district has taken advantage of the empowerment of the sub-county under the decentralization policy to promote and support preventive services.
Table 9: 1995/96 FY SUPPORT PROGRAMS Distribution of vaccines 8 times a month
Cold chain (Storage) monitoring 12 times a month
Contribution to health unit- 8,000 UG.Sh -for primary health care SOURCE: MUKONO DISTRICT 1997 HEALTH PLAN REVIEW
Table 10: 1996/97 FY SUPPORT PROGRAMS Fuel for support supervision (894,000 /-Ug.Sh)
Allowance for support supervision by District Health Team for National immunization days (1,336,400/-Ug.Sh)
Allowance for support supervision- integrated primary health care (710,000/-Ug.Sh)
Allowance for support and supervision (598,140/-Ug.Sh) SOURCE: MUKONO DISTRICT 1997 HEALTH PLAN REVIEW
The second type of support comes in the form of allowances. The district provides allowances for the immunization program. The district health management team receives
additional income when it supervises and supports the sub-county in the vaccination program. These allowances serve as an incentive for better performance.
The third type of support and supervision is related to project selection. The district health committee coordinates the various activities of all health service providers, including NGOs, in the districts. The district health committee can also recommend health projects to be implemented. They help the district in identifying areas and projects that need serious attention. Proposals from the district health committees are sent to the district medical officer for approval. Meetings are then held with NGOs for possible funding. Because of the benefits of attracting NGO projects, the sub-counties try to portray a good picture of themselves, so as
to be in the "good books" of the district health committee.
The tendency to cooperate is derived from anticipated benefits for the parities involved. Katoogo health unit staffs see the need to be responsible to higher authority (the district) in order to earn some kind of financial and technical support, even though they technically have autonomy (Tamale Issa 1997). For example, during 1996/97 FY, the health unit's finances were audited (Mukono Health Quarterly Report 1997). Some observers wonder why finances of a legally autonomous body (sub-county) have to be audited by the district. The district medical officer informed me that supervision and support enhance performance and attract funding (Tumushabe 1997). The district always tries to improve and maintain its
performance in order to provide a rationale for NGO funding; this is very important, since NGOs, such as the District Health Services Project (DHSP), are willing to provide funds for
districts that have been performing well and thus have the ability to use resources effectively. The district is also being guided by the central government to implement projects in line with the national health priority programs. The national health priority programs includes a consolidation of existing services, capacity building, policy enhancement and reorientation to primary health care. These priority areas are the guiding frameworks for health project design and implementation.
A fourth aspect of control from the central government is the policy on drugs. Under this policy, the districts are supposed to buy all their drugs and other medical supplies from designated National Medical Stores (NMS), those licensed by the central government to sell medical supplies to the districts. This drug policy aims at ensuring good quality of drugs at the district health units. In cases where needed supplies are not available at the NMS, districts are given a "Non-Availability Certificate" for purchases in the open market. This policy has
been criticized for contravening the provisions of the decentralization policy, which were stipulated in the Local Statute Act of 1993, but it appears to be working reasonably well.
3. Community Mobilization
Efforts to mobilize the community are done at all levels of government, but the community health workers have been empowered to collect and report all cases of disease within their jurisdiction. They also collaborate with heads of households and the entire community to get information, as described earlier.
Community mobilization has proven to yield a relatively high turnout for immunization. Mobilization of the entire community is now considerably more effective than previously. The sub-county health committee and the community workers are able to reach out to the
remote areas. They also undertake campaigns including home visits, even before national immunization days. The health unit committees ride on bicycles and motorbikes provided by the district, and they sound horns and ring bells to arouse the community's attention.
The field interviews also revealed that the low rates of previous immunization were mainly due to inadequate communication networks and irregular sensitization in these villages. In some cases, ignorance and illiteracy on the part of the mothers have hindered immunization programs. Medical assistants explained that some of the women could not read the dates and other information on the immunization cards given to them. Thus, the mothers
did not even know when to take their children for vaccination. The immunization campaign, as a form of education, has been an effective tool for raising awareness among the
community. The health workers make sure women understand the information on
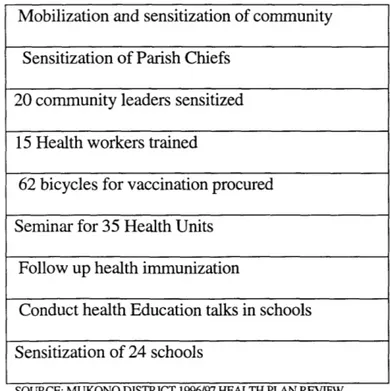
they (women) do not commit themselves to the program. Please see tables 11 and 12 for district and the sub-county collaboration in mobilization activities.
Table 11: 1995/96 FY MOBILIZATION ACTIVITIES
Table 12: 1996/97 FY MOBILIZATION ACTIVITIES Mobilization and sensitization of community
Sensitization of Parish Chiefs 20 community leaders sensitized
15 Health workers trained
62 bicycles for vaccination procured Seminar for 35 Health Units
Follow up health immunization
Conduct health Education talks in schools Sensitization of 24 schools
SOURCE: MUKONO DISTRICT 1996/97 HEALTH PLAN REVIEW Two seminars, 30 community leaders
sensitized
One-day seminar for Head teachers Sensitization of 60 community leaders Carried out 412 outreaches; campaign
Sensitized the LC 3 Chiefs on how to mobilize and motivate community
Because of these mobilization efforts, the response rate on the part of the women has been higher than before. It is evident that the home visits and mobilization have
played a key role in the improved rate of immunization. The vaccination campaign has also raised public awareness; health staff and the entire community have now realized that their inputs for health project planning and implementation should be a primary concern because of the huge externality involved in health. They now know that most of the diseases are contagious and that a collective approach is needed for preventive care. The LC 3 members and the community health workers have played an important
educational role in this area. It must be noted that service provision responsibility devolved to local committees has changed their perception of the environment in which they live. They have complemented self reliance with support and guidance from the higher authorities.
4. High Degree of Flexibility in the Use of Partners in Health Program Implementation at all Levels of Government
Alternative actors, such as NGOs and traditional birth attendants, have been incorporated in the health service provision. NGO representatives now participate in the regular meetings of the district health management team. The district health management team embraces relevant ideas and guidance from the NGOs. Normally, the guidance from the NGOs has concentrated on efficient allocation of resources. The district also supports NGOs in providing services.
Traditional birth attendants were not part of the formal system of health service provision previously. They used to practice in their homes without any supervision and guidance. Now, their contributions have been realized by the district and the sub-county 35
to be very important. The interactions between the traditional birth attendants and the health unit have become more formal. Traditional birth attendants are made to report to the district and they provide information on the number of deliveries that they make. These reports are necessary for identifying children born in the remote villages.
The district now knows the number and distribution of traditional birth attendants and their activities in all the sub-counties. Please see table 13 for the number of deliveries made by the traditional birth attendants in the sub-county as reported to the district
medical office.
Traditional birth attendants list in their reports the names and location of
deliveries. Any problems that arise in the performance of their work are also reported for further action. The health unit relies on this information to follow up on women,
especially in cases of complications that occurred during the time of delivery. This is a kind of maternal child health monitoring that helps to maintain good quality of services not directly offered by the health unit.
One interesting consideration is that the traditional birth attendants are essentially competing with the health units for delivery services. Traditional birth attendants charge
lower prices for their services than the health units. In most cases, the payment of these fees for services can be made in installments. Women sometimes pay for the services in kind. These kinds of payment are flexible and thus make services attractive. With all the competition the health units are facing, they still provide support to the traditional birth attendants to enhance their overall capacity to deliver good services. The incorporation of the traditional birth attendants into the district health system has been necessary because of the workload. The district cannot handle all the needs of the community and therefore
finds it prudent to get some relief from the traditional birth attendants. It is also
sometimes easier for women to go to a nearby traditional birth attendant than to travel all the way to a health center, especially when there is an urgent need for a midwife as women approach labor.
TABLE 13: TRADITIONAL BIRTH ATTENDANT REPORT
NUMBER OF DELIVERIES MONTH 1995 1996 JAN -FEB - 7 MAR - 4 APR - 7 MAY - 8 JUN 3 6 JUL 8 9 AUG 8 -SEP 18 -OCT 7 -NOV 3 -DEC 6 -TOTAL 53 41
Direct support is given to the traditional birth attendants, which is very important because of the implications of their practices for mothers; most of the traditional birth
attendants are untrained. In Uganda, only 39% of women give birth under the care and supervision of trained health workers (Jitta et al.,1996). Traditional birth attendants have been attending meetings and seminars organized by the district. They undergo a series of training sessions to ensure that they maintain a good and hygienic environment when helping women to deliver. Please see Table 14 for the kinds of support and training received by the traditional birth attendants. This support of the traditional birth attendants has been exceptional in Mukono's case, and they, are intum, receptive to new ideas and
guidance provided by the district and the sub-county.
Table 14: SELECTED SUPPORT RECEIVED BY TBAs - 1995/96 FY
ACTIVITY TARGET NO. ACHIEVED
TRAIN 10 TBAs at SSI 10 TBAs 10 TBAS TRAINED
PROCURE/ORDER SUPPLIES 40 PAIR GUMBOOTS 10 PAIR GUMBOOTS
45 BICYCLES 45 BICYCLES
6 CHAIRS,6 TABLES, 6 FORMS, 6 CHAIRS,6 TABLES, 6 FORMS, 6 FILING CABINETS 6 FILING CABINETS
3 FAMILY PLANNING SPACE 3 FAMILY PLANNING SPACE
CREATED CREATED
13 IUD KITS, 2 DELIVERY KITS 13 IUD KITS, 2 DELIVERY KITS
SUPPLIES FOR TBAs PURCHASED 120 DELIVERY
--- KITS FOR TBAs.
TRAINING OF TBAs 24 TBAs 24 TBAs TRAINED
Inter-sectoral collaboration in service delivery has also been very strong. The district medical department shares resources with other departments, such as education, to implement some of their health programs. One example is the use of school teachers in health education programs. These various approaches have strengthened the capacities of
CHAPTER FOUR
4.1 CONCLUSIONS
The dimensions of success identified in the study are generally consistent with emerging findings in recent decentralization literature, some of which is listed in the bibliography. Uganda's major innovations in the health sector include the formation of local health committees, strategic support and supervision from higher levels of
government, expanded community mobilization, and greater flexibility in the use of potential alternative service providers.
1. The Role of Health Committees
One of the most essential prerequisites to effective preventive care is the ability to identify and prioritize problems, which improves the allocation of resources to the
appropriate problem areas (service zones). The study has revealed that newly formed local health committees have performed well in identifying problems in the community. The committees provide the easiest channels to reaching the community, especially in those areas where accessibility is a problem. The village committees are familiar with the intricate pathways that lead to people's compounds. Their knowledge of the village setting has made targeting of health service much easier. The sub-county health
committees use the village health committees to compile health-related information that identifies major problems and vulnerable groups. Key information, such as the number of
children in the village and the incidence of major diseases, is readily made available by these health committees.
The various health committees' interactions (especially that of the health unit management committee with the household heads, local leaders etc.) have enabled them to understand local problems more fully. Preventive health interventions, particularly the vaccination program, have been more effective in rural areas when these intermediaries
are used. The local committees connect the entire community to the district health system; the committees even reach out to the peripheries. This approach has made the provision of services more complete and more integrated.
The integrated health system at Mukono has had a major impact on planning and resource allocation because it is now based on more accurate and comprehensive
information provided by the health committees. The information has helped the district health officers to improve estimates of health problems; conditions of target areas for
immunization are better analyzed, thus helping to make prioritization easier. It was further inferred that underestimation and overestimation of health problems are now reduced compared to before decentralization, because of the improved availability of information about the service zones. Overall, budgeting is now more systematic.
2. Support and Supervision
The accomplishment of the health committees in problem identification would not have been possible without guidance and support from the district. The district's support
and supervision have enabled the health workers to reach out to remote villages. Bicycles provided by the district are used to access the community during collection of data, the mobilization of villages, and the provision of immunization services. Another important form of support is the contribution of medical supplies for immunization. The district
made valuable contributions to the vaccination program by distributing and preserving vaccines.
Other support from the district, which comes in the form of allowances paid to the members of the health committees for all immunization programs, tends to motivate local staff. They become enthusiastic about the whole program and work tirelessly to achieve a high rate of immunization. Allowances that were also given to the supervisors have motivated them. In all the immunization outreach visits, the district provided allowances based on number of visits the health workers made.
The district provides supervision by reviewing local projects. Prioritization and selection of projects for NGO funding has influenced the performance of the sub-county. The sub-counties have been improving their performance and tend to work cooperatively
with the district because of the interest in getting their projects selected for funding. The efforts of the district in preventive care are also complemented by the
guidance from the central government. The district support of the immunization program is provided in line with the national priority areas. The provision of medical supplies to support the sub-county is in accordance with the national policies, and thus serves as a kind of control over the districts. The control of the district by the central government has helped to maintain and improve the quality of services provided in the district.
3. Community Mobilization
It is noteworthy that the sub-county could not have reached their immunization targets without good mobilization and public education programs supported by the district. The district made public awareness, i.e., sensitization programs, one of its
priorities. The study shows an enormous commitment to community mobilization on the part of the district. A number of activities, including sensitization of local council chiefs, parish chiefs and follow-up programs, were carried out. These mobilization activities are among the keys to success.
4. Alternative Service Providers
The capacities of the sub-county and the district to provide good services are partly derived from tapping potential alternative service providers. The district has incorporated both the NGOs and the traditional birth attendants (TBAs) in the health system. NGOs provide the district with supplies and guide them in resource allocation.
The indigenous practice of the traditional birth attendants has not been
suppressed, but rather supported by the district and the sub-county. The promotion of the traditional birth attendants services has been necessary because of the limited capacity of both the sub-county and the district. The TBAs' contributions in the form of reports on newborns has been very essential for preventive health interventions, particularly for achieving the desired vaccination targets.
The collaboration between the traditional birth attendants and the sub-county has evolved to serve the district well, despite the potential competition between them for delivery of services. Cooperation and mutual understanding have played a big part in the
successful performance.
In summary, decentralization has created a conducive environment in Uganda for the provision of more effective preventive health interventions. Local health committees, which have been created within the decentralization system, are the cornerstones of
mobilization; before decentralization, some of the local staff, such as the community health workers, were non-functional. With decentralization, they have been given more power to identify problems, to mobilize the community, and to help in project
implementation. The study has shown that initiative, creativity and flexibility in resource use are the product of higher level control/guidance measures and a willingness to collaborate with alternative service providers.
Despite the success, decentralized health management in Uganda faces a number of unresolved problems. One of the potential problems is the conflict that may arise from the implementation of the national priority areas. Local governments are still tied to the directions of the central government to provide services according to the national
guidelines. This control may undermine local preferences, which the decentralization policy seeks to promote. There are also issues that arise from the assignment of
responsibilities between the sub-county and the district. Sub-county health workers are occasionally confused about what their functions are, since most of the programs sometimes overlap during implementation. However, the local committees now demonstrate potential for bridging this gap because of the training and sensitization programs undertaken in the district. Duties and responsibilities have been outlined more fully for the health workers, but further clarity is required.
4.2 RECOMMENDATIONS
Based on my research, the following recommendations may provide a guide for health service providers and policy-makers in preventive health care.
1) Higher-level support helps the local health committees to perform better and thus should be provided in the implementation of preventive health programs. Support and supervision ensures good standards and helps illuminate areas that need attention. Supervision and support should be part of the overall district health system, if preventive services are to be effective.
2) There is a need to strengthen further the capacities of the health committees in the area of health problem identification because more complete and more
accurate information gathered from local communities has great potential to help the health administrators in making more effective interventions.
3) Training and sensitization programs should be enhanced at all levels of health services administration; this will create an impetus for health program patronage and a capacity to deliver services more effectively.
4) In order to achieve a higher rate of implementation of health programs, alternative service providers in the district should be identified and incorporated into the system. Collaboration with all relevant partners involved in service
provision should be done in such away as to maintain their respective autonomies to the extent possible.
5) Local health committees also need to be more informed about how their collaboration with the districts will benefit them. In a number of the sub-counties visited, some local committee members do not see the value or need to embark on
collaborative programs. They should be made aware of the potential benefits to be derived from joint efforts.
REFERENCES
Aday, Beglay, Larson and Slate. 1996. Evaluating the Medical Care System:
Effectiveness, efficiency and equity. Health Administration Press, Ann Arbor, Michigan. Boissonneau, R. 1986. Health Care Organization and Development. An Aspen
publication. Rockville Maryland Royal Turnbridge Wells.
Burke, Fred G. 1964. Local Government and Politics in Uganda. Syracuse University Press.
Brett, E. A. 1993. Providing for the Rural Poor. Institutional Decay and Transformation in Uganda. Fountain Publishers, Kampala, Uganda.
Fallers, Lloyd A. 1965. Bantu Bureaucracy. A Century of Political Evolution among the Basoga of Uganda . University of Chicago Press.
Holger Bernt, Hanson and Michael Twaddle. 1994. 'From Chaos to Order': The Politics of Constitution Making in Uganda.
Jitta, Kawesa, Kisitu et al., 1996. Evaluation of the Health Financing Reforms in Uganda: A Document Review of User Fees. A paper presented to the World Health Organization Child Health and Development Center, Makerere University, Uganda..
Kasfir, N. 1976. The Shrinking Political Arena. Participation and Ethnicity in African Politics with a case study of Uganda. University of California Press.
Mukono District Health Plan 1995/96.
Mukono District Health Plan Progress Report 1997.
Namunyolo, M.Z. 1986. Health Reforms and Co-production in Africa. Towards Synergy in Uganda Health Care System.
Okuanza and Lubanga 1995. Decentralization and Health Service Systems Change in Uganda. A Report on the Study to Establish Links between Decentralization and Changes in the Health System.
Sabiiti, Justin M. February 19-23, 1996. Implementation of Decentralization Policy. Experiences of Mbara District Political Leadership. A Paper presented at the International Conference on Decentralization in East and West Africa. Kampala.
Sathyamurthy,T.V. 1992. Central-Local Relations. The Case of Uganda. University of Manchester.
Siegel Bruce, Peters David and Kamara Sheku 1996. Health Reform in Africa. Lessons from Sierra Leone. World Bank discussion paper No.347. The World Bank,Washington D.C. pp 1-22.
Smith, Richard, A. 1978. Manpower and Primary Health Care. The University Press of Hawaii Honolulu.
Soren, Villadsen and Lubanga Francis 1996. Democratic Decentralization in Uganda: A New Approach to Local Governance. Fountain Publishers Ltd. Kampala Uganda.
Sorkin, Alan, L. 1976. Health Economics in developing Countries. Lexington Books, D.C. Heath and Company, Lexington Massachusetts.
Tamale Issa. (Katoogo Medical Assistant, Uganda). Interview on 7-30-97. The Three Year Health Plan Frame 1993/94. The Government of Uganda.
Tumushabe, E.K (Mukono District Medical Officer, Uganda). Interview on 7-9-97. Uganda Local Government Act, 1993.
Uganda Local Government Act, 1997.
United Nations. 1994a. Department of International and Social Affairs.World Population Prospects. New York.
United Nations Department for Policy Coordination and Sustainable Development. 1994. Cooperative Enterprise in the Health and Social Care Sectors. A Global Survey,.
New York.
United States Bureau of the Census 1994(BUCN). International Data Base Version. Van, Thomas, T.H. 1995. Analysis and Evaluation of Health Care Systems .Health Professions Press, Baltimore.