Risks to Young Volunteers in International Social Projects
11
0
0
Texte intégral
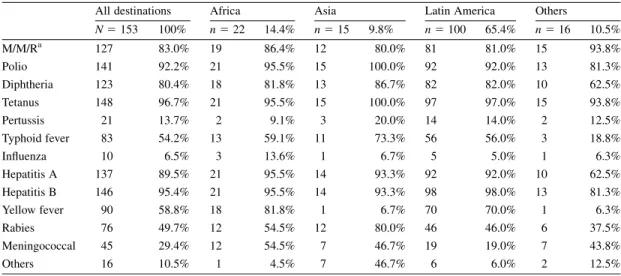
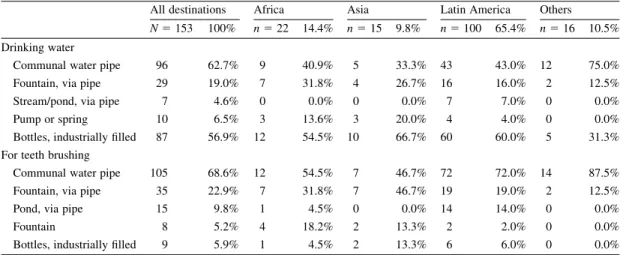
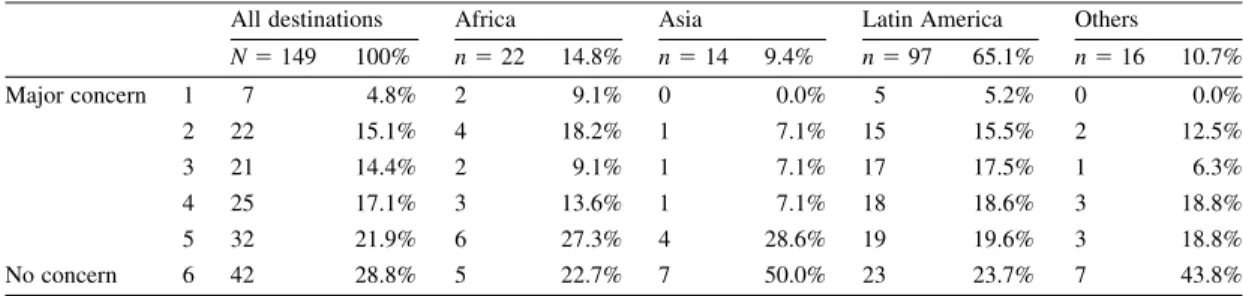
Figure

+2
Documents relatifs