Publisher’s version / Version de l'éditeur:
Proceedings Graphics Interface 2012, pp. 69-75, 2012-06-01
READ THESE TERMS AND CONDITIONS CAREFULLY BEFORE USING THIS WEBSITE. https://nrc-publications.canada.ca/eng/copyright
Vous avez des questions? Nous pouvons vous aider. Pour communiquer directement avec un auteur, consultez la première page de la revue dans laquelle son article a été publié afin de trouver ses coordonnées. Si vous n’arrivez pas à les repérer, communiquez avec nous à [email protected].
Questions? Contact the NRC Publications Archive team at
[email protected]. If you wish to email the authors directly, please see the first page of the publication for their contact information.
NRC Publications Archive
Archives des publications du CNRC
This publication could be one of several versions: author’s original, accepted manuscript or the publisher’s version. / La version de cette publication peut être l’une des suivantes : la version prépublication de l’auteur, la version acceptée du manuscrit ou la version de l’éditeur.
Access and use of this website and the material on it are subject to the Terms and Conditions set forth at
Cybersickness induced by desktop virtual reality
Vinson, Norman G.; Lapointe, Jean-Francois; Parush, Avi; Roberts, Shelley
https://publications-cnrc.canada.ca/fra/droits
L’accès à ce site Web et l’utilisation de son contenu sont assujettis aux conditions présentées dans le site LISEZ CES CONDITIONS ATTENTIVEMENT AVANT D’UTILISER CE SITE WEB.
NRC Publications Record / Notice d'Archives des publications de CNRC:
https://nrc-publications.canada.ca/eng/view/object/?id=aa9661c8-91d9-49d9-bb47-a27a194e454f
https://publications-cnrc.canada.ca/fra/voir/objet/?id=aa9661c8-91d9-49d9-bb47-a27a194e454f
Cybersickness Induced by Desktop Virtual Reality
ABSTRACT
Cybersickness, a syndrome resulting from exposure to virtual reality displays, raises ethical and liability issues. We have found that, contrary to the majority of previous reports in the literature, cybersickness can be induced by desktop virtual real-ity. Moreover, our findings suggest that some individuals sus-ceptible to cybersickness can be screened out on the basis of their self-reported susceptibility to motion sickness.
KEYWORDS: Cybersickness, simulator sickness, screening,
desktop, liability, ethics.
INDEX TERMS: K.4.1 [Computers and Society]: Public Policy
Issues — Ethics, Human safety; H.1.2 [Models and Principles]: User/Machine Systems — Human factors, Experimentation; I.3.7 [Computer Graphics]: Three-Dimensional Graphics and Realism — Virtual reality, Experimentation.
1 INTRODUCTION
Cybersickness (also known as virtual reality sickness or simula-tor sickness) is a syndrome that can arise from the use of Virtual Reality (VR) technology. Cybersickness has three major symp-tom clusters: nausea, oculomotor discomfort, and disorientation [15]. The symptoms manifest themselves to varying degrees as a function of several variables, including (but not limited to) dis-play technology [23], exposure time [33], and individual suscep-tibility [23], [5].
Understandably, cybersickness is not very pleasant and most people would wish to avoid it. From the perspective of the indi-vidual consumer, cybersickness is likely a disincentive to using VR technology. From a business perspective, cybersickness raises liability issues for VR devices, limiting the desire of com-panies to produce VR products. Moreover, from a business adoption standpoint, what company would want to use technol-ogy that makes their employees sick? Cybersickness is essen-tially a barrier to both adoption and production of VR technolo-gies [3], [8], [14], [34]. Consequently, an understanding of cy-bersickness and of ways to minimize it could help further the growth and acceptance of VR.
11200 Montreal Road, M50, Ottawa, ON, Canada K1A 0R6;
{norm.vinson | jean-francois.lapointe}@nrc-cnrc.gc.ca
2
B552 Loeb Building, 1125 Colonel By Drive, Ottawa, ON, Canada, K1S 5B6; [email protected]
31135 Innovation Drive, Suite 300. Ottawa (Kanata), Ontario
Canada K2K 3G7 [email protected]
Cybersickness also raises ethical issues [2], relating in part to the central research ethics principle of beneficence [29]. In re-search ethics, beneficence encourages rere-searchers to maximize the benefits of experiments while minimizing their harms (and risks thereof), particularly with respect to the experiment’s par-ticipants. In the context of beneficence, cybersickness is a poten-tial harm. To increase beneficence then, researchers should minimize the risk, incidence, and severity of cybersickness. The ethics implications of cybersickness are particularly relevant for researchers in Australia, Canada, and the USA, since many of them are required to have their experiments approved by a re-view board mandated to ensure compliance with research ethics guidelines. These review boards will certainly be concerned about the beneficence, and therefore the risk of cybersickness, of any VR experiments. Moreover, the risk of cybersickness should lead these boards to require greater benefits and methodological rigor from VR studies than from lower risk studies [29].
In this paper, we present our findings that desktop VR pro-duces cybersickness. While cybersickness has been found to result with a variety of display types, there has been little exami-nation of the effects of desktop VR on cybersickness. We de-scribe an experiment in which we presented desktop VR and measured cybersickness levels using the Simulator Sickness Questionnaire [15].
In addition, we discuss the performance of a screening ques-tionnaire in identifying individual participant characteristics that indicate susceptibility to cybersickness. Such a questionnaire could be used by virtual reality researchers to further reduce the risk of cybersickness by screening out the more susceptible par-ticipants.
Before turning to our results, we present a brief discussion of the symptoms and causes of cybersickness.
1.1 Cybersickness Symptoms and Measurement
Distinctions can be made between the symptoms of cybersick-ness and simulator sickcybersick-ness. Generally, cybersickcybersick-ness is more severe, and tends to have a relatively more important disorienta-tion component. Nonetheless, the range of symptoms is substan-tially the same [33]. Consequently, in the following discussion we will not distinguish between simulator sickness and cyber-sickness.
Perhaps the best place to begin an examination of cybersick-ness symptoms is the Simulator Sickcybersick-ness Questionnaire (SSQ) developed by Kennedy, Lane, Berbaum, and Lilienthal [15]. The SSQ was based on the Pensacola Motion Sickness Questionnaire because simulator sickness symptoms resembled those of mo-tion sickness. The symptoms included in the SSQ are listed in Table 1 below. These symptoms are grouped into three major components: nausea, oculomotor discomfort, and disorientation.
Norman G. Vinson1 Jean-François Lapointe1 Avi Parush2 Shelley Roberts3
National Research Council, Canada
National Research Council, Canada
Table: 1 SSQ Symptoms. Some of the symptoms are included in more than one subscale. nIndicates nausea sub-scale symptoms, oindicates oculomotor discomfort symptoms, and dindicates disorientation symptoms.
1.2.2 Vection
Vection is a sensation of self-motion produced by visual stimu-lation. More vection results in greater sensory conflict. Accord-ingly, conditions that produce greater vection also increase cy-bersickness. Specifically, environments with more objects and more detailed texture maps will lead to a stronger perception of self-motion during navigation, and consequently, result in more cybersickness. (In contrast, consider navigating through a com-pletely black environment. There is no perception of motion and no cybersickness) [30].
An increase in avatar velocity also increases vection, produc-ing more cybersickness [30], [25].
Even a change in vection seems to increase cybersickness [4]. 1.2.3 Apparatus Characteristics
Some factors that are related to particular types of displays have also been found to produce cybersickness. Head lag and jitter are particularly associated with Head Mounted Displays (HMDs). The orientation of the viewpoint on the virtual scene is tied to the HMD, such that a change in head orientation will produce a corresponding change in viewpoint orientation. The position trackers required to perform this operation are not per-fect, resulting in jitter — small but high frequency movements of the viewpoint. Lack of processing speed or latency in head position acquisition result in head lag — a delay between head movement and the corresponding screen update. Both head lag and jitter have been found to cause cybersickness [23].
Stereo glasses provide a more compelling experience of depth by presenting slightly different images to each eye, requiring the brain to fuse the images in a way that produces a perception of depth. Unfortunately, such a display can place unnatural de-mands on the visual system [27]. It is perhaps not surprising then that stereo glasses have been found to increase nausea when incorporated into a HMD [19].
1.2.4 Individual Differences
Several studies show that there are substantial differences be-tween individuals in their susceptibility to cybersickness (for example [5]). Individual difference factors affecting cybersick-ness include age, with older individuals being more susceptible [25]; gender, with females having experienced more cybersick-ness in some studies [26], and even differences related to optoki-netic nystagmus (OKN), a visuo-motor response to visual mo-tion tracking [9].
Still more factors have been found to influence cybersickness [26]. Considering all factors, we should expect that, on the whole, desktop displays would induce the least amount of cyber-sickness because they incorporate the fewest causative factors. Desktop displays that do not use position trackers will not pro-duce jitter or head lag. If stereo glasses are not used, their cyber-sickness-inducing properties will not be a factor. Finally, desk-top displays can result in less sensory conflict. The field of view is small enough that users do not perceive motion in their visual periphery. This peripheral stability is consistent with the stabil-ity of the user’s body, and so may reduce sensory conflict, thus reducing cybersickness. Consequently, we would expect that desktop displays would induce less cybersickness than other VR display technologies.
1.3 Cybersickness Induced by Desktop VR
Most of the research on cybersickness focuses on immersive displays (such as HMDs, BOOMs, simulators, and large screens), with little examination of desktop VR-induced cyber-sickness [5], [21], [33]. There are anecdotal reports that desktop VR does not cause cybersickness (e.g. [12], [36], [35]) and some general discomfortno fatigueo headacheo
difficulty focusingod sweatingn eye straino
fullness of headd nauseand blurred visionod
increased salivationn vertigod dizzy (eyes open)d
stomach awarenessn burpingn dizzy (eyes closed)d difficulty concentratingno
Additional, perhaps more worrisome, symptoms have been reported in the literature: flashbacks [16], vomiting [23], and postural instability [23]. Moreover, symptoms can linger on following the exposure to VR [33], [32].
In the SSQ, the severity of each symptom is indicated by the participant using a four-point scale composed of none, slight, moderate and severe, which are respectively scored 0, 1, 2, and 3 [15], [18]. The scores are summed across symptoms for each subscale, and a coefficient is applied to each sum to provide each subscale measure. The SSQ is computed by removing the coefficients from the subscale scores, summing the resulting quotients and multiplying that sum by 3.74 [15]1.
Each of the SSQ symptoms can appear with a variety of se-verities, or not at all, depending on several factors, not the least of which is individual susceptibility [23], [5].
Despite being developed to assess simulator sickness (as the name suggests), a 2001 review reports that 40 out of 50 studies on cybersickness used the SSQ as a cybersickness measure [30]. Subsequent to 2001, the SSQ has continued to be used in cyber-sickness studies and it now constitutes a defacto standard.
Below we examine some of the factors that modulate the se-verity of cybersickness to introduce our experiment dealing with the relation between desktop displays and cybersickness.
1.2 Factors Affecting Cybersickness Severity
The prevailing, though not universally accepted, physiological explanation for cybersickness is the sensory conflict theory. According to this theory, visual sensory information suggesting that the body is moving conflicts with vestibular sensory infor-mation (from the inner ear) suggesting that the body is stable. This conflict produces cybersickness [23], [5]. Accordingly, increasing sensory conflict worsens cybersickness, the particu-lars of which are laid out below.
1.2.1 Exposure Time
For example, increasing the time the sensory conflict lasts by prolonging exposure worsens cybersickness [26], [33], [17]. However, cybersickness has been found to decrease when an individual is exposed over multiple sessions. This suggests an adaptation to the sensory conflict [17].
1
The sum must be executed before the multiplication to match the examples in Table 6 of Kennedy et al.’s SSQ article [15].
measure cybersickness in only a very cursory manner (e.g. [1]). Nonetheless, most of the sources we found indicate that we should not expect cybersickness to result from exposure to desk-top VR. More specifically, we should expect mean post expo-sure SSQs of about 5 to 15 ([5], [7], [28], and our own prior work.) Nonetheless, a few researchers have found post SSQ scores of only 15 to be statistically different from pre-exposure desktop VR SSQ scores [28], [20].
In the experiment described here, we found a much greater final SSQ of 25, and a high pre/post SSQ difference of nearly 18. Our study clearly shows the potential for desktop VR to cause cybersickness.
2 METHOD
It is important to note that the primary purpose of our study was to examine the effects of different input devices and device-to-avatar motion mappings on virtual walkthrough performance. This is reflected in the study design discussed below, and pre-sented in more detail in [22].
Participants used four different travel techniques for their virtual walkthroughs. By technique, we mean a particular com-bination of an input device, a number of hands used to control the device, a number of degrees of freedom, and a device-to-avatar movement mapping. Each technique moved the device-to-avatar and viewpoint together, such that the avatar’s viewpoint always faced in the same direction as the avatar’s forward motion. In all cases, a rate control algorithm controlled the translations of the viewpoint in the VE.
The first travel technique involved using a standard 104 key keyboard to control 3 motion degrees of freedom (DOF): fore/ aft and left/right translation and rotation along the horizontal plane, around the vertical axis (yaw). Speed was constant at 5 m/s for translations, and 180°/s for rotations.
The second travel technique was based on a mouse. Here, the lateral, side-to-side, movement of the mouse rotated the view-point along the horizontal plane, around the vertical axis (yaw). Rotation speed was determined by an algorithm with a linear function gain of 25° of rotation per cm of lateral mouse move-ment (with mouse acceleration disabled). The left and right but-tons controlled the fore/aft movement at a constant speed of 5 m/s. Thus, the mouse travel technique had only two DOFs: one translation and one rotation.
The third travel technique involved a 3-DOF joystick as the input device. A lateral tilt of the joystick resulted in a lateral displacement of the viewpoint, while forward/backward joystick tilt produced a fore/aft movement of the viewpoint. Finally, a twist of the joystick’s handle rotated the viewpoint on the hori-zontal plane, around the vertical axis (yaw). Translation speed was controlled through a linear function gain up to a maximum speed of 5 m/s. Rotational speed was a constant 180°/s.
The fourth and final travel technique employed a gamepad with two mini joysticks to control 2 translation DOFs and one rotation DOF. As with the 3D joystick, a lateral tilt of the left joystick produced a lateral movement of the viewpoint. A fore-word/backward tilt of the left joystick produced the fore/aft movement of the viewpoint. Unlike the 3D joystick, the horizon-tal plane rotation, around the vertical axis, (yaw) was controlled by the second joystick. Translation speed had proportional ve-locity control with a linear function gain, to a maximum of 5 m/s. The rotation speed was a constant 180°/s.
We measured trial completion times, virtual distance trav-elled, number of collisions, and subjective preferences.
We leveraged the opportunity of conducting this VR naviga-tion study to also assess cybersickness and its relanaviga-tion to our
screening questionnaire. To assess cybersickness we had partici- Figure 2: Bird’s-eye-view perspective on the
environ-ment .
Figure 1: Environment from avatar’s perspective.
pants fill out the SSQ just before starting the experiment and after using each one of the four different travel techniques.
2.1 Participants
The participants were recruited via an email message sent to the employees of a large government research lab. Of the 34 partici-pants who volunteered for the experiment, 8 were unable to complete it due to cybersickness, and 2 participants were re-moved to create a balanced latin square design. Of the 2, we removed one male participant to retain one female participant who had experienced the conditions in the same order. This provided us with a better gender balance of 10 females and 14 males. The other removed subject was selected randomly.
This left 24 participants that corresponded to the 24 travel technique presentation order permutations, producing a properly counterbalanced experiment.
All participants were computer literate, had at least a high-school-level education, and normal or corrected-to-normal vi-sion. Their average age was 36.
2.2 Display Apparatus
The system included a color desktop monitor with a diagonal size of 54 cm and a resolution of 1600x1200 pixels. The frame rate was 60 Hz, with system latency less than 120 ms. The par-ticipant’s viewing distance was 70 cm. The avatar had a radius of 0.25 m, a viewing height of 1.8 m, and a field of view of 75° x 60° (H x V). The virtual trail was 2 m wide with walls that were 3 m high and obstacles that were 1 m high, thus allowing the participants to see over them. The corridor was 164.5 m long (measured along the centerline), with 15 turns to the right and 15 to the left. Note that the top part of the screen is black, and that the blue and green maze barriers are not texture mapped. The scene complexity is therefore relatively low (see Figures 1 and 2).
2.3 Task
Participants had to complete a primed search task, where they knew in advance the target location. They were instructed to travel from the start point to the end point in the shortest time possible (Figure 2).
Each participant used each of the four travel techniques to accomplish their task.
2.4 Design
The independent variables were the four travel techniques de-scribed above and the dependent variables were the task comple-tion time, the total traveled distance and the number of colli-sions. We used a within-subject design and trials were blocked by travel technique. We counterbalanced the order in which participants used each travel technique to minimize skill transfer effects. Order counterbalancing attributed any exposure time effects on the SSQ evenly to each interface.
For each travel technique (each block), the participants re-ceived brief explanations by the experimenter, followed by 2 practice trials and 5 experiment trials.
2.5 Procedure
This experiment met the exacting standards of, and was ap-proved by, the Canadian National Research Council’s Research Ethics Board. Participants completed a consent form before participation. They were also informed that they could stop the experiment at any time to take a break or withdraw.
To reduce the risk of cybersickness, potential participants who were not experiencing their typical level of fitness or health were asked not to volunteer [19]. A pre-experiment question-naire included statements related to fitness and health along with other criteria ostensibly indicative of a propensity to motion sickness, dizziness, or eyestrain (see Table 2)
Participants also filled out a pre-experiment SSQ. They were then seated in front of the apparatus and began the experiment. The instructions were displayed on-screen before each trial. A 3-second audio countdown preceded each trial. The trials ended automatically when the participants reached the ending point. Once all trials for one travel technique were completed, partici-pants filled out another SSQ, and then began the next block of trials. After all blocks were completed, participants filled out a final SSQ and completed a post-test survey to rate each travel technique.
Average exposure time was 35s per trial, about 4 minutes per block, and 16 minutes total. The whole experiment took about an hour, but this included instructions and time taken by filling out the various forms.
3 RESULTSAND DISCUSSION
Our results fall into two categories: desktop induced cybersick-ness and the relationship between our screening questionnaire and individual susceptibility to severe cybersickness.
3.1 Desktop Induced Cybersickness
Recall that we had participants fill out the SSQ before the ex-periment and after each 4-minute block of trials.
Our analysis of the SSQ data follows previous cybersickness studies that have subjected SSQ scores to ANOVAs or t-tests (e.g. [26], [17], [18]). However, the latin square design makes it impossible to calculate the interaction between trial blocks and interface type. Consequently, we conducted two separate ANOVAs: one gender by interface type ANOVA, and one gen-der by trial block ANOVA. Note that trial block is a proxy for exposure time, each block lasting about 4 minutes.
Only trial block had a significant effect on SSQ scores F (4,88)=8.3, p<0.001 (which remains significant even if we apply a Bonferroni correction for having run two separate ANOVAs, making the alpha level 0.025 [6]). The subscales also showed the same pattern of results: a significant main effect only for trial block. F(4,88)=8.7, p<0.001 for nausea; F(4,88)=5.1, p<0.002 for oculomotor discomfort; and F(4,88)=6.9, p<0.001 for disorientation.
While the different travel techniques did have a significant effect on walkthrough performance (see [22]), they did not have a significant effect on cybersickness.
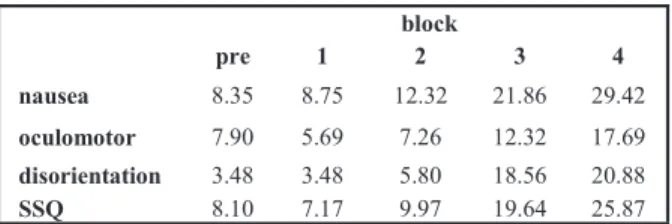
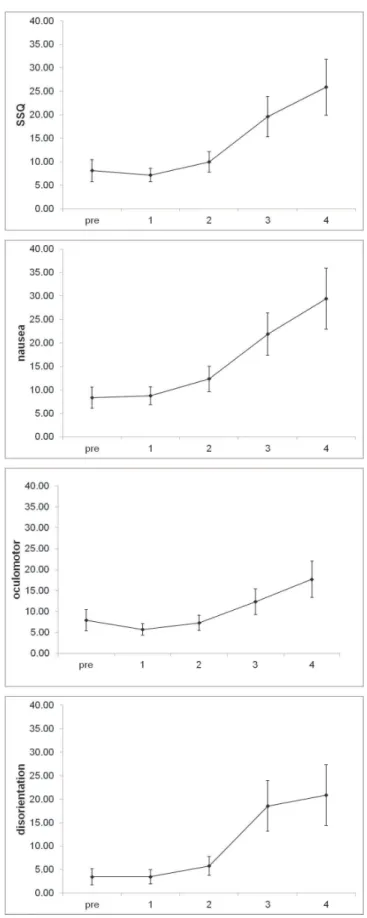
Cybersickness does not appear until after the third trial bloc, which was equivalent to about 12 minutes of exposure. Figure 3 shows the effect of trial block on SSQ and subscale scores, while Table 3 provides the average scores.
Our desktop VR caused cybersickness. Moreover, after about 12 minutes of exposure, the average SSQ score exceeded 15. An analysis of SSQ scores resulting from simulator use indicates that a score above 15 is a concern, while scores above 20 indi-cate a bad simulator [33]. While it has previously been shown that desktop VR displays generally produce less cybersickness than immersive displays [5], [11], our scores are in the range of
# Statements (True/False) Source
1 I am ill 1
2 I am tired or lack sleep 1
3 I am under the influence of drugs and/or
alcohol 1
4 I have a hangover 1
5 I have an upset stomach 1
6 I am under unusual stress 1
7 I am susceptible to sickness induced by
video or computer games 2
8 I suffer from dizzy spells 3
9 I have had an ear infection in the last 10
years 3
10 I get motion sickness 2
11 I wear glasses with progressive correction
or a powerful prescription 3
12 I wear contact lenses 3
Table 2: Ostensible cybersickness susceptibility state-ments. 1‑Health/fitness related (based on [19]), 2-suggested by [13], 3-ad hoc.
block pre 1 2 3 4 nausea 8.35 8.75 12.32 21.86 29.42 oculomotor 7.90 5.69 7.26 12.32 17.69 disorientation 3.48 3.48 5.80 18.56 20.88 SSQ 8.10 7.17 9.97 19.64 25.87 Table 3: SSQ and subscale average scores before ex-posure (pre) and following each trial block.
those produced by immersive displays [21], [33].
In addition, 23.5% of the participants who began the experi-ment were unable to finish due to excessive cybersickness. (Their data is not included in the above analyses.) This drop out rate even exceeds that from some immersion studies [21].
This experiment caused more cybersickness than has been reported before with desktop displays (see section 1.3). Indeed, one of the authors routinely travels in virtual environments with little cybersickness. However, he was unable to complete this experiment while serving as a pilot subject. Why then was this experiment so much more sickening than those reported previ-ously? There are five possibilities:
1 Exposure time
2 Visual complexity of the environment 3 Travel speed
4 Number, extent, and speed of rotations 5 Something else
We can see the effect of exposure time in Figure 3. After the second block of trials, cybersickness can still be characterized as minimal, yet it becomes concerning after the third block [33]. However, this only represents about 12 minutes of exposure time. Unfortunately, it is difficult to determine whether exposure time accounts for our findings since most desktop VR studies do not report it.
So and colleagues [30] have shown that visual complexity of the environment and travel speed (translation or rotation) are both related to vection, which itself is related to cybersickness. Our environment however was not very complex (Figure 1): almost half the screen was blank and much of the rest was not even texture mapped. Furthermore, our rate of translation was low because of the sharp turns required of the avatar.
However, both the rate of rotation and the angle of rotation were high in comparison to studies on rotation and cyber/motion sickness [25], [26], [31], [37]. In addition, our experiment re-quired 15 90° right turns and 15 90° left turns per trial, each of which lasted about 35s. Of the first four candidates mentioned above, we can speculate that such rapid, extensive, and frequent rotations are the most likely culprit for the cybersickness we observed. However, the relationship between rotation and cyber-sickness is not straightforward [30]. For example, there appears to be an inverted U-shaped relationship between rotation veloc-ity and cybersickness such that cybersickness peaks between 30 and 60 deg/s [31]. Since our rotation velocities were much higher than those used in [31], it is difficult to assess their ef-fects on cybersickness. Moreover, it isn’t completely clear that rotations are inherently more cybersickness-inducing than trans-lations. Consequently, additional research is required to more fully assess the effects of different forms of avatar motion on cybersickness. In particular, a wider range of translational and rotational velocities should be studied, as well as a greater range of rotation angles, in the context of virtual environment naviga-tion.
This leads us to the fifth possibly: something else. Investigat-ing this possibility will require even more research.
3.2 Individual Susceptibility
The discomfort of cybersickness has led to a call for methods to identify highly susceptible individuals so they can avoid VR [31]. In this context, researchers found that individual differ-ences in a component of optokinetic nystagmus (OKN) were related to cybersickness susceptibility. However measuring this OKN component is not very convenient, as it requires an eye tracker [9].
Figure 3: Total SSQ and subscale scores as a func-tion of trial block.
environment [10], [38]. These latter metaphors, particularly those involving much less viewpoint motion, should lead to less visual/proprioceptive sensory conflict. It is therefore possible that such metaphors like the scene in the hand or the eyeball in
the hand [10], [38] are less cybersickening than walkthroughs
and flythroughs. Consequently, readers should be wary of ex-tending our findings to 3D interaction metaphors whose view-points are situated outside the virtual environment.
REFERENCES We endeavored to find a simpler way of identifying
indi-viduals at high risk for cybersickness. Reviewing the litera-ture, we found that motion sickness history has been shown to correlate with simulator sickness [13] (which, while not iden-tical to cybersickness, is nonetheless related [33]). We there-fore devised a short questionnaire that included self-reported susceptibility to motion sickness and cybersickness. We also included other items (#1 to #6) related to health and fitness, and other items that could indicate a propensity for dizziness and/or nausea (see Table 2).
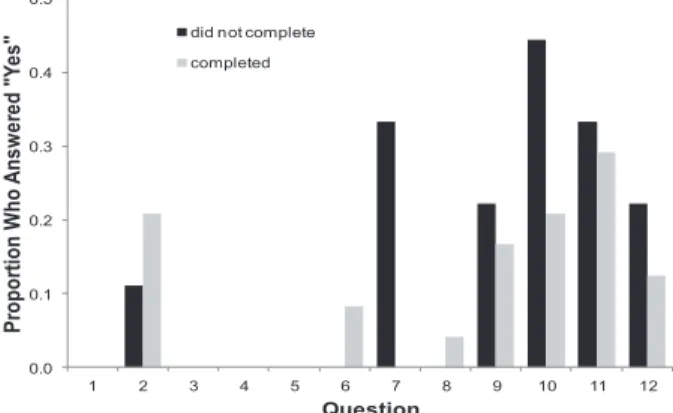
To analyze our questionnaire’s effectiveness in predicting the cybersickness of individuals, we divided the participants into two groups: those who were able to complete the experi-ment, and those who had to stop due to the severity of their cybersickness symptoms. Examining the response to the ques-tions as a function of group membership showed that only the motion sickness and cybersickness susceptibility questions (#7 and #10) discriminated between the two groups (see Fig-ure 4). Indeed, a Chi square test pooling the responses to questions 7 and 10 showed a significant difference between the two groups (χ2(1)=4.65 (corrected for continuity), p=0.03). There was no confound with gender as the effect of gender on the distribution of participants in the completed/did not complete groups was not significant: χ2(1)=0.03 (or 0.00 if corrected for continuity), p=1.
We did not expect questions #1 to #6 to discriminate be-tween the groups since our call for participation screened out those who would have responded positively.
4 CONCLUSIONS
Cybersickness is a serious impediment to the adoption of VR [3], [8], [14]. Yet cybersickness induced by desktop VR has received little attention. Our study shows that desktop VR can indeed cause cybersickness.
To reduce the occurrence of cybersickness in future studies we endeavored to find a simple method of screening out par-ticipants who are more likely to be susceptible to cybersick-ness. We found that self-reported susceptibility to cyber and motion sickness can indentify participants who will have to withdraw from the experiment due to severe cybersickness. If a few more studies corroborate our findings, researchers should be able to use this characteristic to reduce the risk of cybersickness in future VR experiments.
As noted earlier, another topic for further research involves the role of different types of viewpoint motions and speed in cybersickness. We noted that our environment contained sev-eral sharp turns per trial and that the viewpoint rotations needed to negotiate these turns may have been responsible for the excess cybersickness our participants experienced. How-ever, the relationship between viewpoint motion and cyber-sickness is not straightforward [4], [30].
One possible factor affecting cybersickness is the sharpness of the turn. A gentle turn along an arc may have less effect on cybersickness than a sharp turn on the spot despite both turns effecting the same orientation change. The difference is not the total rotation executed but rather how “sharp” it is (see [24] for a related study).
One should note that the experiment described here in-volved a virtual walkthrough metaphor. In both walkthrough and flythrough metaphors, the viewpoint is embedded in the environment [10]. In these metaphors, the viewpoint moves through the environment, resulting in a visual/proprioceptive sensory conflict, which is thought to underlie cybersickness [23]. However, there are other metaphors of interaction with 3D environments wherein the viewpoint is situated outside the
Figure 4: Proportion of participants who agreed with the statements shown in Table 2, grouped by whether they were able to complete the experiment.
[1] R. W. Allen, D. Fiorentino, E. Viirre. Novice driver training results and experience with a PC based simulator. In proceed-ings of the Second International Driving Symposium on Human Factors in Driver Assessment, Training and Vehicle Design (Park City, Utah, USA), pp. 165-170, 2003.
[2] K. M. Behr, A. Nosper, C. Klimmt, and T. Hartmann. Some practical considerations of ethical issues in VR research. Pres-ence: Teleoperators and Virtual Environments, 14:668-676, 2005.
[3] F. Biocca. Will simulation sickness slow down the diffusion of virtual environment technology? Presence: Teleoperators and Virtual Environments, 1:334-343, 1992
[4] F. Bonato, A. Bubka, S. Palmisano, D. Phillip, Moreno, G. Vection change exacerbates simulator sickness in virtual envi-ronments, Presence: Teleoperators and Virtual Envienvi-ronments, 17:283-292, 2008.
[5] S. V. G. Cobb, S. Nichols, A. Ramsey, and J. R. Wilson. Vir-tual-reality induced symptoms and effects (VRISE), Presence: Teleoperators and Virtual Environments, 8:169-186, 1999. [6] A. Field. Discovering Statistics Using SPSS for Windows.
Sage. 2000.
[7] R. Garris-Reif, T.M. Franz. Simulator sickness and human task performance in conventional and virtual environments. In A.C. Bittner, P.C. Champney (Eds.), Advances in Industrial Ergo-nomics and Safety VII, Taylor & Francis, 1995.
[8] N. Gross. Seasick in cyberspace, Business Week, pp. 110-111, July 10, 1995.
[9] C. Guo, J. Ji, R. So. Could OKAN be an objective indicator of the susceptibility to visually induced motion sickness? In pro-ceedings of IEEE Virtual Reality Conference (Singapore, March, 19-23, 2011). Pp. 87-90, 2011. 0.0 0.1 0.2 0.3 0.4 0.5 1 2 3 4 5 6 7 8 9 10 11 12 Pr o p o rti o n W h o A n s w e re d " Y e s " Question
did not complete completed
[10] C. Hand. A Survey of 3D Interaction Techniques. Computer Graphics Forum, 16:269–281, 1997.
[11] C. Johns. Spatial Learning: Cognitive mapping in abstract virtual environments. In proceedings of AFRIGRAPH '03 The 2nd International Conference on Computer Graphics, Virtual Reality, Visualisation and Interaction in Africa. (Cape Town, South Africa), pp. 7-16, 2003.
[12] N. Katz, H. Ring, Y. Naveh, R. Kizony, U. Feintuch, P.L. Weiss. Interactive virtual environment training for safe street crossing of right hemisphere stroke patients with unilateral spatial neglect. In proceedings of 5th International Conference on Disability, Virtual Reality & Associated Technologies (Oxford, UK, 2004) pp. 51-56, 2004.
[13] R.S. Kennedy, J.E. Fowlkes, K.S. Berbaum, M.G. Lilienthal. Use of a motion sickness history questionnaire for prediction of simulator sickness. Aviation, Space and Environmental Medi-cine, 63:588-593, 1992
[14] R.S. Kennedy, K.E. Kennedy, K.M. Bartlett. Virtual environ-ments and products liability. In K.M. Stanney, editor, Hand-book of Virtual Environments: Design, Implementation and applications, pages 543-554. CRC press, 2002.
[15] R. S. Kennedy, N. E. Lane, K. S. Berbaum, and M.G. Lilien-thal. Simulator sickness questionnaire: An enhanced method for quantifying simulator sickness. International Journal of Aviation Psychology, 3:203-220, 1993.
[16] R.S. Kennedy, N. E. Lane, M.G. Lilienthal, K. S. Berbaum, and L.J. Hettinger. Profile analysis of simulator sickness symptoms - Application to virtual environment systems. Presence: Teleoperators and Virtual Environments, 1:295-301, 1992 [17] R.S. Kennedy, K.M. Stanney, W.P. Dunlap. Duration and
Exposure to Virtual Environments: Sickness Curves During and Across Sessions. Presence: Teleoperators and Virtual Environments, 9:463-472, 2000.
[18] E. M. Kolasinski, and R. D. Gilson. Simulator sickness and related findings in a virtual environment. Proceedings of Hu-man Factors and Ergonomics Society 42nd Annual Meeting (Chicago, IL, USA, Oct. 5-9, 1998). pp. 1511-1515, 1998. [19] E. M. Kolasinski, S. L. Goldberg, and J. H. Hiller. Simulator
Sickness in Virtual Environments, Technical Report 1027, Army project # 20262785A791. U.S. Army Research Institute for the Behavioral and Social Sciences, Department of the Army, 1995.
[20] D.R. Lampton, J.P. Gildea, D.P. McDonald, E.M. Kolasinski. Effects of Display Type on Performance in Virtual Environ-ments, Technical Report 1049, Army project # A790. U.S. Army Research Institute for the Behavioral and Social Sci-ences, Department of the Army, 1996.
[21] D.R. Lampton, E. M. Kolasinski, B.W. Knerr, J.P. Bliss, J.H. Bailey, B.G. Witmer. Side effects and aftereffects of immersion in virtual environments. In proceedings of Human Factors and Ergonomics Society 38th Annual Meeting (Nashville, TN, USA, Oct. 24-28, 1994). pp 1154-1157, 1994.
[22] J.-F. Lapointe, P. Savard, N.G. Vinson. A Comparative Study of Four Input Devices for Desktop Virtual Walkthroughs. Com-puters in Human Behavior, 27, 2186-2191, 2011
[23] J. J. LaViola. A discussion of cybersickness in virtual environ-ments. SIGCHI Bulletin, 32:47-56, 2000.
[24] J. J. W. Lin, H. Abi-Rached, and M. Lahav. 2004. Virtual guiding avatar: an effective procedure to reduce simulator sickness in virtual environments. In proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI '04) (Vienna, Austria), pp.719-726, 2004
[25] C.-L. Liu, S.-T. Uang. Measurement and Prediction of Cyber-sickness on Older Users Caused by a Virtual Environment. In C. Stephanidis, editor, Universal Access in Human-Computer Interaction, Ambient Interaction, Lecture Notes in Computer Science, Volume 4555/2007, 666-675, 2007
[26] W.T. Lo, R.H.Y So. Cybersickness in the presence of scene rotational movements along different axes. Applied Ergonom-ics, 32:1-14, 2001
[27] M. Mon-Williams, and J. P. Wann. Binocular virtual reality displays: When problems do and don't occur. Human Factors, 40:42-49, 1998.
[28] S. Sharples, S. Cobb, A. Moody, J.R. Wilson. Virtual reality induced symptoms and effects (VRISE): Comparison of head mounted display (HMD), desktop and projection display sys-tems. Displays, 29:58-69, 2008.
[29] J. A. Singer, and N. G. Vinson. Ethical issues in empirical studies of software engineering. IEEE Transactions on Soft-ware Engineering, 28:1171-1180, 2002.
[30] R.H.Y So., A. Ho, W.T. Lo. A Metric to Quantify Virtual Scene Movement for the Study of Cybersickness: Definition, Implementation, and Verification. Presence: Teleoperators and Virtual Environments, 10:193-215, 2001.
[31] R.H. So, H. Ujike. Visually induced motion sickness, visual stress and photosensitive epileptic seizures: what do they have in common? Applied Ergonomics, 41:491-493, 2010
[32] K. M. Stanney, and R. S. Kennedy, Aftereffects from virtual environment exposure: How long do they last? In proceedings of the Human Factors and Ergonomics Society 42nd Annual Meeting (Chicago, IL, Oct. 5-9, 1998), pp. 1476-1480, 1998. [33] K. Stanney, R. S. Kennedy, and J. M. Drexler. Cybersickness is
not simulator sickness. In proceedings of the Human Factors and Ergonomics Society 41st Annual Meeting (Albuquerque, NM, USA, Sept. 22-26, 1997). pages 1138-1142, 1997. [34] K. M. Stanney, and G. Salvendy. Aftereffects and sense of
presence in virtual environments: Formulation of a research and development agenda. International Journal of Human-Computer Interaction, 10:135-187, 1998.
[35] A. Tait. Desktop virtual reality. Proceedings of IEE Collo-quium on Using Virtual Worlds (London, UK, Apr. 15, 1992). pp. 5/1-5/5, 1992.
[36] F. Tyndiuk, G. Thomas, V. Lespinet-Najib, and C. Schlick. Cognitive Comparison of 3D Interaction in Front of Large vs. Small Displays. In proceedings of VRST (Virtual Reality Soft-ware and Technology) (Monterey, CA, USA, Nov. 7-9, 2005) pp. 117-123, 2005.
[37] H. Ujike, T. Yokoi, S. Saida. Effects of virtual body motion on visually-induced motion sickness. In proceedings of Engineer-ing in Medicine and Biology Society, 2004 (IEMBS '04) (San Francisco, CA, USA, Sept. 1-5, 2004), pages 2399-2402, 2004. [38] C. Ware, S. Osborne. Exploration and virtual camera control in
virtual three dimensional environments. Computer Graphics, 24:175-183, 1990