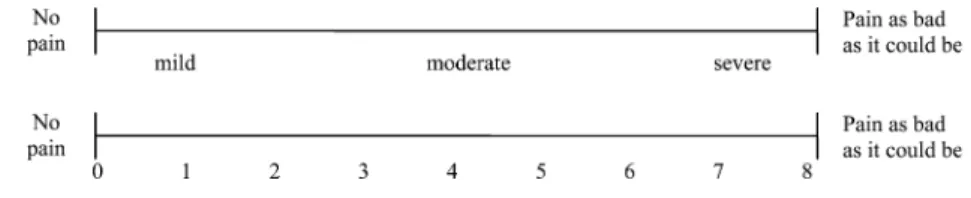
Pain assessment
8
0
0
Texte intégral
Figure
Documents relatifs
Texte intégral
Figure
Documents relatifs
