p53 protein expression but not mdm-2 protein expression is associated with rapid tumor cell proliferation and prognosis in renal cell carcinoma
6
0
0
Texte intégral
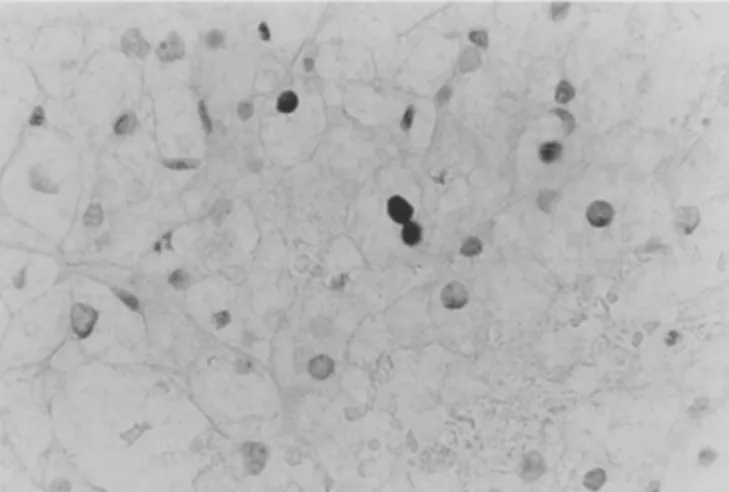
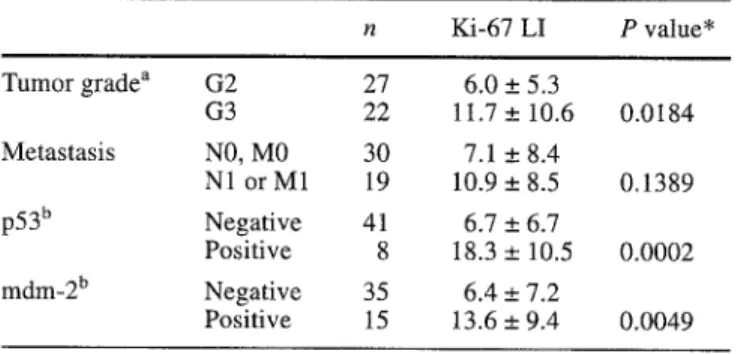
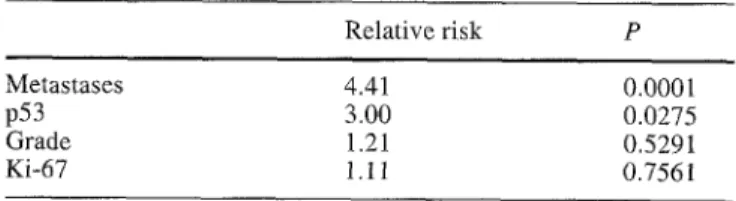
Figure
Documents relatifs