View of IMPROVING TEACHING THROUGH CROSS COLLEGE COLLABORATION: REFLECTIONS ON A SASKATCHEWAN EXPERIENCE
22
0
0
Texte intégral
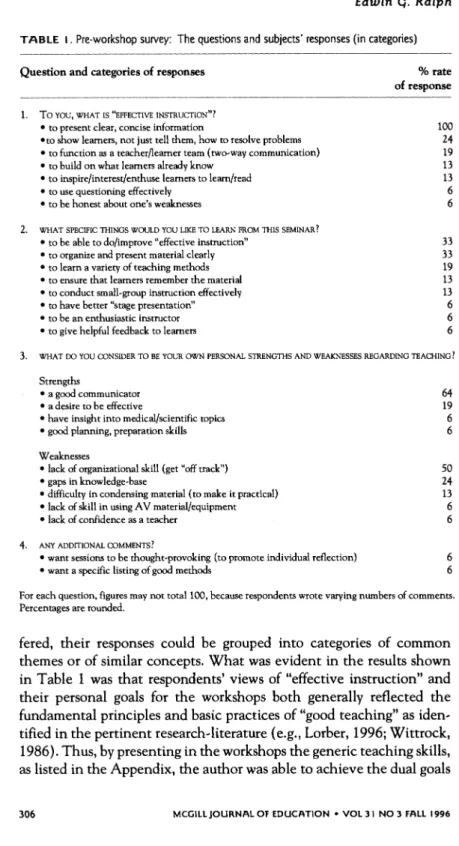
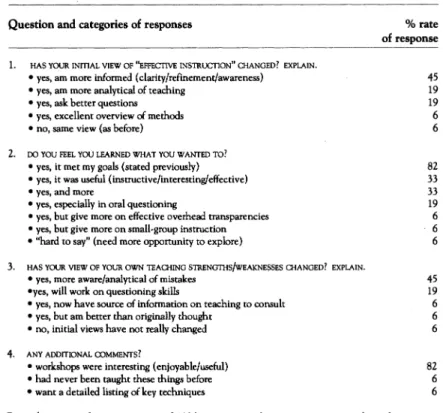
Figure
Documents relatifs