Endothelin receptor antagonists: a place in the management of essential hypertension?
4
0
0
Texte intégral
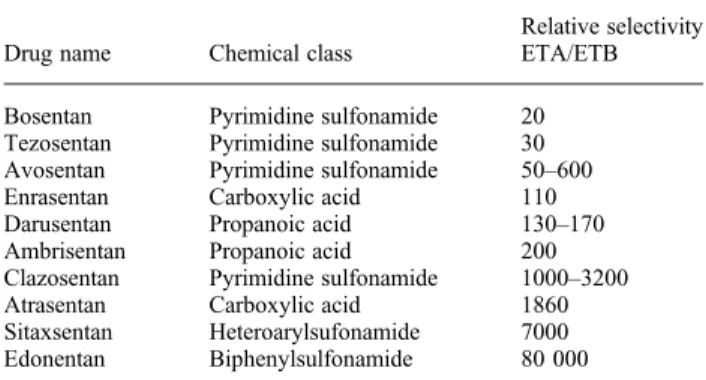
Figure
Documents relatifs
