ORIGINAL ARTICLE
Effect of ozone on periodontopathogenic
species
—an in vitro study
Sigrun Eick&Marius Tigan&Anton Sculean
Received: 9 September 2010 / Accepted: 18 January 2011 / Published online: 2 February 2011 # Springer-Verlag 2011
Abstract The in vitro study was aimed to determine the effect of ozone on periodontopathogenic microorganisms. Ozone was generated for 6 s–2×24 s (corresponding to 0.56 mg–2×2.24 mg of ozone) against 23 mainly anaerobic periodontopathogenic species. Agar diffusion test was used as a screening method. Then, the killing activity was tested in a serum-free environment and with 25% v/v inactivated serum. Further, the effect of ozone on bactericidal activity of native serum was analyzed against Fusobacterium nucleatum, Porphyromonas gingivalis, and Aggregatibacter actinomycetemcomitans. Agar diffusion test showed a high efficacy of ozone against microorganisms, especially against Porphyromonas gingivalis. This result was con-firmed by the killing tests; most of the strains in a concentration of 105 were completely eliminated after twofold 18-s application of ozone. Only four of the six potentially “superinfecting” species (Staphylococcus aure-us, Enterococcus faecalis, Enterobacter cloacae, Candida albicans) survived in part. Addition of heat-inactivated serum reduced the killing rate of ozone by 78% after 6-s and by 47% after twofold 18-s exposures; no strain was completely eradicated after any application of ozone. The bactericidal effect of native serum was enhanced after application of ozone; no effect was visible on the included A. actinomycetemcomitans strain which was found to be completely resistant to the bactericidal action of serum. In conclusion, (a) ozone has a strong antibacterial activity against putative periodontopathogenic microorganisms, and (b) the bactericidal effect is reduced in the presence of
serum. Ozone may have potential as an adjunctive application to mechanical treatment in periodontitis patients.
Keywords Ozone . Periodontitis . Anaerobes . Serum
Introduction
Periodontal disease status impacts markedly on biofilm composition [1]. It is generally accepted that a small group of predominantly gram-negative anaerobic or microaero-philic bacteria is associated with initiation and progression of periodontitis. Organisms strongly implicated as etiologic agents of periodontitis include Aggregatibacter actino-mycetemcomitans, Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola [2]. Moreover, other species such as Campylobacter rectus, Eubacterium noda-tum, Fusobacterium nucleanoda-tum, Prevotella intermedia, Parvimonas micra, and Streptococcus constellatus support pathogenesis of disease. Eikenella corrodens, enterobac-teria, Pseudomonas spp., Selenomonas spp., and yeasts may play a role as superinfecting species [2, 3]. Nowadays, dental implants are widely used. Similar microbial patterns like in periodontitis are found in periimplant diseases [4,5]. Subgingival bacterial biofilms are surrounded by gingival crevicular fluid (GCF), which is rich of serum [6]. Serum may inhibit efficacy of antimicrobials [7]. Contrary, bactericidal activity of complement being a constituent of native serum is a well-known mechanism in innate immunity.
Based on the impact of pathogens, antiinfective regimen is an important component in any treatment of periodontal and periimplant diseases. In preventing recolonization of bacteria, chlorhexidine digluconate is a widely used agent in periodontitis treatment [8,9]. Antibiotics are recommended
S. Eick (*)
:
M. Tigan:
A. SculeanDepartment of Periodontology, University of Bern, Freiburgstrasse 7,
CH-3010 Bern, Switzerland e-mail: [email protected]
for severe cases [10, 11]. As an alternative method, application of laser is discussed [12]. Another possibility might be ozone. Ozone is a naturally occurring compound consisting of three oxygen atoms. It is a powerful antimicro-bial agent by destructing cell walls and cytoplasmic mem-branes of bacteria and fungi [13–15]. In vitro, ozone is active against salmonella contaminations on food, Escherichia coli, Pseudomonas aeruginosa, Staphylococcus aureus, Aspergil-lus fumigatus, and Candida albicans. Ozone can enhance serum-mediated killing of bacteria [16].
As reviewed recently by Azarpazhooh and Limeback [17], application of ozone might be promising as a prophylactic antimicrobial prior to restorations and as a denture cleaner, contrary in vitro data are conflicting regarding endodontics, oral and maxillofacial surgery, oral diseases as well as implant therapy. Nearly nothing is known about application of ozone in treatment against periodontopathogens. Only one study using ozonated water showed a killing effect on A. actinomycetemcomitans and Porphyromonas gingivalis in vitro [18].
Therefore, the aims of the in vitro study were: (a) to determine the effect of ozone on microorganisms which are involved in the pathogenesis of periodontitis and periimplantitis and (b) to evaluate the possible influence of serum on the antibacterial efficacy of ozone.
Material and methods
The Prozone® device which is CE labeled (W&H, Bürmoos, Austria) was used according to the manufac-turer’s description. The manufacturer obligates the usage of an evacuation system with a power of 50 L/min at the application site; nevertheless, the device should be not used in patient having pacemakers and respiratory problems or in pregnant women. Times of 6, 12, 18, and 24 s were applied by using the Coro tips always in a distance of 2 mm to the surface. By using Coro tips, 140 ppm of ozone per minute is produced corresponding to 2.24 mg of ozone per 24 s. In periodontology, 18-s applications are recommended by the manufacturer. Controls were not exposed to any ozone. Microorganisms
At a total, 23 different microbial strains were included in the study. Seventeen of these strains belong to species clearly involved in pathogenesis of periodontitis; the six others may play a role as potentially superinfecting species. The periodontopathogens were grouped into Porphyromo-nas gingivalis strains, A. actinomycetemcomitans strains, gram-positives as well as other gram-negatives. Three Porphyromonas gingivalis strains, three A. actinomycetem-comitans strains as well as two potentially superinfecting
species originated from clinical samples obtained from patients with severe periodontitis (Table1).
All the strains were precultivated 24–72 h prior to the experiments. Modified tryptic soy agar [19] and trypic soy agar (BD, Franklin Lakes, NJ, USA) were used as cultivation media. A. actinomycetemcomitans strains and the Streptococcus constellatus ATCC 27823 were always incubated with 5% CO2, all potentially superinfecting species within normal atmospheric conditions and the other periodontopathogens anaerobically (80% N2, 10%CO2, 10% H2), each at 37°C. The number of bacteria was adjusted to OD640nm=0.1 which refers to 1.5×10
8
bacterial cells/mL. These suspensions were diluted to the necessary concentration in the experiments.
Agar diffusion test as a screening method
First, a defined amount of microbes (105) was spread on Wilkins-Chalgren agar plates (BD) and Mueller-Hinton agar plates (BD) respectively. For that, the suspension McFarland 0.5 was diluted 1:150, and each 100μl is used. Prozone device using the Coro tips was placed in a distance of about 1–2 mm to the surface of the agar. Ozone was applied for 18 and 24 s. Further, in one case, the device was kept on its place and the spot of microorganisms was exposed to ozone for a second time (2×24 s). One part of the plate served as growth control. After an incubation time of 42 h (18 h aerobes), the effects including diameters of the inhibition zones were registered.
Quantitative killing activity of ozone on different microorganisms
A defined inoculum of microorganisms (105 and 103 in 10μl NaCl 0.9% each) was given into 1.5-mL tubes. After a short centrifugation, the tubes were placed for 15 min in the laminar air flow to enable a bacterial layer containing a reduced amount of liquid. A complete dryness as recom-mended by the manufacturer was avoided; this would not represent an in vivo situation. Ozone was applied for 6, 12, 18, and 24 s. Two tubes were exposed to ozone for a second time (2×18 s and 2×24 s) and two served as controls (no exposure to ozone). The numbers of colony-forming units (cfu) were determined after addition of 100μl NaCl 0.9% solution, mixing, serial dilution, and plating each 25μl on agar plates and incubation in the appropriate atmosphere. Influence of serum as an essential component
of GCF on killing activity
Determinations of killing activity were repeated in the presence of 25% v/v serum (Sigma-Aldrich, Steinheim, Germany). Serum was heat-inactivated (30 min at 56°C) to
exclude the bactericidal effect by complement. In these experiments, only two times (6 s, 18 s) and one repeated exposure (2×18 s) as well as one microbial concentration (105) were used in dependence of the results obtained before in determination killing activity of ozone without serum.
Effect of ozone on serum-mediated killing on selected bacterial species
Selected bacterial species (Porphyromonas gingivalis ATCC 33277, A. actinomycetemcomitans J7, F. nucleatum ATCC 25586; each 107/10μl NaCl 0.9%) were exposed for 12 s to ozone before addition of 100μl serum 25% v/v in NaCl 0.9% solution. The used higher microbial concentra-tion was necessary to achieve about 105 viable cells after treatment with ozone. After an incubation of 15 min at 37°C in an anaerobic atmosphere, the numbers of cfu were determined. NaCl 0.9% solution with inactivated serum as well as samples without exposure to ozone served as controls.
All experiments were made in independent duplicates at least. Statistical analysis was made by using paired Student’s t test and ANOVA with post-hoc Bonferroni.
Results
Agar diffusion test
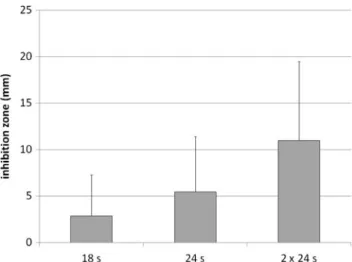
In mean, the diameters of the inhibitions zones were 2.87 ± 4.42 mm after an application of ozone for 18 s, 5.41 ± 5.84 mm for 24 s, and 11.0 ± 8.49 mm for the twofold 24-s application of ozone (Fig. 1). Inhibition zones with > 20 mm were found against four strains by using the highest exposure of ozone. No inhibition was seen against 15 strains by using the lowest exposure, 10 strains after the moderate exposure, and three strains after the highest exposure of ozone, respectively. The highest inhibition zones were measured after exposing ozone against Porphyromonas gingivalis and the smallest were observed on the plates with capnophilic and anaerobic gram-positive bacterial strains (data not shown).
Killing by ozone
Ozone was efficient in killing the tested microorganisms. In mean, the killing rate was more than 90% after exposure times of 12 s for 103 and 18 s for 105 microorganisms (Fig. 2). A significant difference between the two used
Species Origin Group
Porphyromonas gingivalis ATCC 33277 Laboratory strain Porphyromonas gingivalis P. gingivalis M5-1-2 Clinical isolate Porphyromonas gingivalis P. gingivalis MaRL Clinical isolate Porphyromonas gingivalis P. gingivalis J430-1 Clinical isolate Porphyromonas gingivalis Aggregatibacter actinomycetemcomitans
ATCC 33384
Laboratory strain Aggregatibacter actinomycetemcomitans A. actinomycetemcomitans J1 Clinical isolate Aggregatibacter actinomycetemcomitans A. actinomycetemcomitans J2 Clinical isolate Aggregatibacter actinomycetemcomitans A. actinomycetemcomitans J7 Clinical isolate Aggregatibacter actinomycetemcomitans Campylobacter rectus ATCC 33238 Laboratory strain Other gram-negatives
Capnocytophaga gingivalis ATCC 33624 Laboratory strain Other gram-negatives Eikenella corrodens ATCC 23834 Laboratory strain Other gram-negatives Fusobacterium nucleatum ATCC 25586 Laboratory strain Other gram-negatives Prevotella intermedia ATCC 25611 Laboratory strain Other gram-negatives Tannerella forsythia ATCC 43037 Laboratory strain Other gram-negatives Eubacterium nodatum ATCC 33099 Laboratory strain Gram-positives Parvimonas micra ATCC 33270 Laboratory strain Gram-positives Streptococcus constellatus ATCC 27823 Laboratory strain Gram-positives
Enterobacter cloacae JGr1 Clinical isolate Potentially“superinfecting” strains Klebsiella pneumoniae JGr2 Clinical isolate Potentially“superinfecting” strains Pseudomonas aeruginosa DSM 50071 Laboratory strain Potentially“superinfecting” strains Enterococcus faecalis ATCC 29212 Laboratory strain Potentially“superinfecting” strains Staphylococcus aureus ATCC 29213 Laboratory strain Potentially“superinfecting” strains Candida albicans ATCC 76615 Laboratory strain Potentially“superinfecting” strains Table 1 Tested microorganisms
concentrations of the microbial strains was not found at any exposure time.
Following, only results using the 105 microorganisms are presented.
Ozone completely eradicated most of the strains in a concentration of 105 after twofold 18-s application of ozone. Only four of the six potentially “superinfecting” species survived in part (Table2).
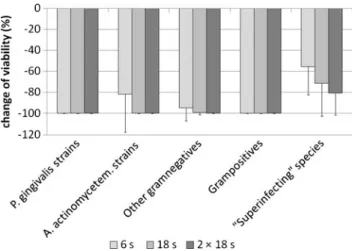
Porphyromonas gingivalis was killed after any applica-tion of ozone. A. actinomycetemcomitans was eliminated nearly completely after 18-s exposure of ozone. The other gram-negative anaerobic and capnophilic periodontopathic strains were also highly susceptible to ozone. Only in tests with 105of F. nucleatum ATCC 25586, the twofold 18- or 24-s application of ozone was necessary to eradicate totally that strain. The gram-positive anaerobic and capnophilic periodontopathic strains were killed to 100% by ozone in general. The potentially “superinfecting” species were less sensitive to ozone. Most resistant were the Enterobacter cloacae JGr1 and the gram-positive bacterial strains (killing rates of 105microorganisms and twofold 18-s exposure to ozone: Enterobacter cloacae JGr1 51%, Enterococcus faecalis ATCC 29212 76%, Staphylococcus aureus ATCC 2921 62%). Further, Candida albicans ATCC 76615 survived in part after the twofold 18-s exposure to ozone (killing rate 94%). The results for 6 s, 18 s as well as 2×18 s of exposure to ozone are presented in Fig.3; at all time-points, differences between the microbial groups were significant (6 s: p=0.002; 18 s: p=0.035; 2×18 s: p=0.037).
Killing in the presence of serum
Although adjusting the same concentration at the beginning of the experiments, cfu counts were higher in the control samples with serum showing a protective influence of serum on viability of bacteria. Addition of inactivated serum reduced clearly the killing rate of all selected bacterial strains by ozone. No strain was completely eradicated after any application of ozone. The killing rate was descreased by 78% after 6-s and by 47% after twofold 18-s exposures to ozone (each p<0.001). Twofold 18-s application enhances the killing of ozone compared to onefold usage (killing rate for all strains after twofold 18-s application, 50 ±25%; after onefold 18-s application, 34±26%; p<0.001; Fig.4).
Also the killing rate of Porphyromonas gingivalis was lowered in the presence of serum. Nevertheless, 72% of the bacteria were killed after exposure of twofold 18 s of ozone. Contrary to Porphyromonas gingivalis, only 50% of A. actinomycetemcomitans and of the included other gram-negative anaerobic and capnophilic periodontopathic strains were killed after twofold 18-s exposure of ozone. Serum also reduced the efficacy of ozone against gram-positive capnophilic and anaerobic periodontopathic bacteria by about 40%. After the twofold 18-s application of ozone, only 28% of the microbial cells of the potentially super-infecting species were killed in the presence of serum (Figs.3and4). Most resistant was Candida albicans ATTC 76615 (11%), followed by the gram-positives (Enterococcus faecalis ATCC 29212 (27%), Staphylococcus aureus ATCC 2921 (28%)) and Klebsiella pneumoniae JGr2 (27%); more sensitive were the Pseudomonas aeruginosa
Fig. 2 Changes in viabilities of microorganisms (mean and standard deviation) by different time of exposure to ozone for all tested micro-organisms. Ozone was applied to 103and 105microorganisms/10μl 0.9%
NaCl in tubes for 6, 12, 18, and 24 s as well as 2×18 and 24 s (24 s corresponds to 2.24 mg of ozone). The references were microorganisms without exposure to ozone (median controls: 1,220 cfu for testing 103 microorganisms and 79,000 cfu for testing 105). The numbers of cfu were determined after addition of 100μl NaCl 0.9% solution and plating different dilutions on agar plates
Fig. 1 Inhibition zones (mean and standard deviation) for all tested microbial strains after exposure of 16 s, 24 s as well as 2×24 s to ozone (24 s corresponds to 2.24 mg of ozone). Microbes were spread on agar plates. Prozone device was placed in a distance of about 1–2 mm to the surface. After application of ozone and an incubation time of 42 h (18 h aerobes) the effect including diameters of the inhibition zones were registered
DSM 50071 (38%) and the Enterobacter cloacae JGr1 (39%) strains.
Effect of ozone on bactericidal activity of serum
First, microbial concentration and exposure time of ozone had to be chosen which did not destroy all cells. In using Porphyromonas gingivalis ATCC 33277 and F. nucleatum ATCC 25886, bactericidal killing of serum was enhanced after application of ozone. No effect was visible on A. actinomycetemcomitans J7 which was found to be resistant to any effect of serum (Table3).
Discussion
Ozone is used for different purposes in medicine. It may reduce acute back pain [20] and inflammation in venous ulcer [21]. Ozone is widely used for disinfection of drinking water; it can inactivate influenza viruses [22], bacilli [23], and Escherichia coli [24]. In dentistry, ozone was discussed in endodontic treatment since 1951 [25]; nevertheless, clinical studies are missing. Ozone was found to prevent white spot lesions in orthodontic patients [26]
and to stop or reverse fissure and root caries lesions [27,
28]. Knowledge about a possible usage of ozone in periodontitis and periimplantitis is extremely limited.
Here, the effect of ozone on periodontopathogens was studied. As shown by agar diffusion test and confirmed by the killing assays, ozone was highly efficient in combating these species. Species-specific aspects were found. Ozone was more active against the major periodontopathogens, compared to the potentially super-infecting species. Especially, Porphyromonas gingivalis was very susceptible to the action of ozone. Although expecting a toxic effect of oxygen molecules against anaerobes or capnophilic species, data about an efficacy of ozone against anaerobes or capnophilic species are extremely rare. Nagayashi et al. [18] studied the effect of ozonated water on selected oral species; the included Porphyromonas gingivalis strain was extremely sensitive and even more than oral streptococci and A. actinomycetemcomitans. Thus, our results referring the relation Porphyromonas
Fig. 4 Influence of 25% v/v serum (inactivated) on changes in viabilities (mean and standard deviation) by 105by 6 s, 18 s as well as
2×18 s of exposure to ozone for all tested microorganism (18 s corresponds to 1.68 mg of ozone). Ozone was applied to 105
microorganisms per 10 μl NaCl 0.9% with 25% v/v serum. The references were microorganisms without exposure to ozone (median of 79,000 cfu without serum and 174,000 cfu with serum). The numbers of cfu were determined after addition of 100μl NaCl 0.9% solution and plating different dilutions on agar plates. The respective results without serum are shown in Fig.2
Fig. 3 Changes in viabilities (mean and standard deviation) of different groups of microorganisms in concentrations of 105by 6 s, 18 s as well as 2×18 s of exposure to ozone (18 s corresponds to 1.68 mg of ozone)
Group of microbes (number of strains) Application of ozone
6 s 12 s 18 s 2×18 s 24 s 2×24 s P. gingivalis (4) 4 4 4 4 4 4 A. actinomycetemcomitans (4) 0 2 3 4 3 4 Other gram-negatives (6) 4 5 5 6 5 6 gram-positives (3) 2 2 3 3 3 3 “Superinfecting” species (6) 0 1 2 2 2 2
Table 2 Number of strains (105microorganisms) which were totally killed after different times of exposure to ozone
gingivalis and A. actinomycetemcomitans and using gas-eous ozone confirm this. Another study found Parvimonas micra as a species involved in root canal infections to be highly susceptible [29]. The destroying potential of radical ions of oxygen as another oxygen species was more pronounced on F. nucleatum, Porphyromonas gingivalis, and Prevotella intermedia than on Streptococcus sobrinus [30].
The potential superinfecting species, especially the gram-positive species Staphylococcus aureus and Enterococcus faecalis as well as Candida albicans, were less sensitive in general. Data about a slightly higher efficacy of ozone against Pseudomonas aeruginosa in comparison to Staphylococcus aureus and Enterococcus faecalis [31] were confirmed. In another study, Enterococcus faecalis was found to be less sensitive to ozone than to common disinfectants [32]. In endodontic infections where Enterococcus faecalis is a critical species [33], the effect of ozone was limited in an ex vivo model [34].
Gingival crevicular fluid contains up to 35% of the albumin found in serum [35]. Serum proteins may bind to antimicrobials and, following this, inhibit the activity of different antibiotics [36] and disinfectants [37]. Bacteria can use serum as a nutrient source [38] which may explain higher cfu counts of controls in experiments with serum. Data about the influence of serum on the activity of ozone are different. Ten percent bovine fetal serum did not interfere with the activity of ozone [31]; whereas 5–10%
of human plasma reduced in a concentration-dependent manner the killing activity of ozone [39]. Our results also clearly indicate that efficacy of ozone is decreased in the presence of 25% v/v human serum, but still killing was found up to 90% in dependence of the strain, especially after a twofold 18-s application of ozone (Fig.5).
Serum proteins might be essential compounds of subgingival biofilm matrix which are highly organized and adapted communities [40]. Although in this study the efficacy of ozone on biofilms was not tested, a limited effect can be assumed. It has been shown that ozone kills moderately efficiently cariogenic bacteria in saliva [41] and the effect is minimal in a cariogenic biofilm using saliva as protein source [42]. Further studies are needed to evaluate the possible effect of ozone against periodontopathogenic bacteria within biofilm. The reduced antibacterial activity of ozone in the presence of serum together with its
anticipated limited effect against microorganisms within biofilm may suggest the adjunctive application of ozone to mechanical therapy in periodontitis patients.
An enhanced bactericidal activity of serum as described before [16], probably due to membrane damage by ozone leading to a more rapid penetration of the membrane attack complex of complement [43] was found for two of the three strains. Complement was found to be activated within gingival fluid [44], suggesting a possible clinical relevance of the findings. The third included strain, A. actinomycetemcomitans J7, was highly resistant against serum; this did not change after the application of ozone. Resistance of many periodontopathogens against killing by complement is well known [45, 46]; a complete resistance is probably not abolished by ozone.
It may be also suggested that ozone influences host response. Host response to biofilm plays a critical role in the pathogenesis of periodontitis [47]; many proinflammatory cytokines are involved in inflammation and bone loss [48]. Resolution of inflammation may be supported by ozone; ozone was found to inhibit NFκB-pathways [49] as well to increase the phagocytotic capacity of bovine PMNs in inflammation [50]. Ozone was shown to be toxic to human oral epithelial cells and gingival fibroblasts but in a lower extent than different antimicrobials [51]. The possible modulatory properties of host response by ozone might be
Fig. 5 Influence of 25% v/v serum (inactivated) on changes in viabilities of different groups of microorganisms in concentrations of 105 by 6 s, 18 s as well as 2×18 s of exposure to ozone (18 s corresponds to 1.68 mg of ozone)
Bactericidal effect of serum without ozone (%)
Bactericidal effect of serum with ozone (%)
P. gingivalis ATCC 33277 21.15±4.53 61.90±13.47
A. actinomycetemcomitans J7 −12.62±17.25 −20.04±17.21
F. nucleatum ATCC 25886 22.59±28.81 86.24±3.81
Table 3 Serum-mediated killing without and after 12-s application of ozone
of importance in periodontitis and should be specified in vitro and in vivo in this context.
Based on the present findings, it can be concluded that: (a) ozone has a strong antibacterial activity against anaerobic periodontal pathogenic microorganisms, (b) the bactericidal effect is reduced in the presence of serum, and, following, (c) ozone may have potential as an adjunctive application to mechanical treatment in periodontitis patients.
Acknowledgments The authors are grateful to Regula Hirschi and Marianne Weibel for excellent assistance in performing the in vitro assays. This study was supported by W&H (W&H, Bürmoos, Austria). Conflict of interest The authors declare that they have no conflict of interest.
References
1. Socransky SS, Haffajee AD (2005) Periodontal microbial ecology. Periodontol 2000 38:135–187
2. Consensus report (1996) Periodontal diseases: pathogenesis and microbial factors. Ann Periodontol 1:926–932
3. Socransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Jr (1998) Microbial complexes in subgingival plaque. J Clin Periodontol 25:134–144
4. Hultin M, Gustafsson A, Hallstrom H, Johansson LA, Ekfeldt A, Klinge B (2002) Microbiological findings and host response in patients with peri-implantitis. Clin Oral Implants Res 13:349–358 5. Van de Velde T, Thevissen E, Persson GR, Johansson C, De Bruyn H (2009) Two-year outcome with Nobel Direct implants: a retrospective radiographic and microbiologic study in 10 patients. Clin Implant Dent Relat Res 11:183–193
6. Schenkein HA, Genco RJ (1977) Gingival fluid and serum in periodontal diseases. I. Quantitative study of immunoglobulins, complement components, and other plasma proteins. J Periodontol 48:772–777
7. Selk SH, Pogany SA, Higuchi T (1982) Comparative antimicrobial activity, in vitro and in vivo, of soft N-chloramine systems and chlorhexidine. Appl Environ Microbiol 43:899–904
8. Santos S, Herrera D, Lopez E, O'Connor A, Gonzalez I, Sanz M (2004) A randomized clinical trial on the short-term clinical and microbiological effects of the adjunctive use of a 0.05% chlorhexidine mouth rinse for patients in supportive periodontal care. J Clin Periodontol 31:45–51
9. Cosyn J, Sabzevar MM (2007) Subgingival chlorhexidine varnish administration as an adjunct to same-day full-mouth root planing. II. Microbiological observations. J Periodontol 78:438–445 10. van Winkelhoff AJ, Winkel EG (2009) Antibiotics in periodontics:
right or wrong? J Periodontol 80:1555–1558
11. Guentsch A, Jentsch H, Pfister W, Hoffmann T, Eick S (2008) Moxifloxacin as an adjunctive antibiotic in the treatment of severe chronic periodontitis. J Periodontol 79:1894–1903
12. Tomasi C, Schander K, Dahlen G, Wennstrom JL (2006) Short-term clinical and microbiologic effects of pocket debridement with an Er:YAG laser during periodontal maintenance. J Periodontol 77:111–118
13. Das E, Gurakan GC, Bayindirli A (2006) Effect of controlled atmosphere storage, modified atmosphere packaging and gaseous ozone treatment on the survival of Salmonella Enteritidis on cherry tomatoes. Food Microbiol 23:430–438
14. Murakami H, Mizuguchi M, Hattori M, Ito Y, Kawai T, Hasegawa J (2002) Effect of denture cleaner using ozone against methicillin-resistant Staphylococcus aureus and E. coli T1 phage. Dent Mater J 21:53–60
15. Dyas A, Boughton BJ, Das BC (1983) Ozone killing action against bacterial and fungal species; microbiological testing of a domestic ozone generator. J Clin Pathol 36:1102–1104
16. Doroszkiewicz W, Sikorska I, Jankowski S (1993) Ozone as sensitizer of bacteria to the bactericidal action of complement. Acta Microbiol Pol 42:315–319
17. Azarpazhooh A, Limeback H (2008) The application of ozone in dentistry: a systematic review of literature. J Dent 36:104–116 18. Nagayoshi M, Fukuizumi T, Kitamura C, Yano J, Terashita M,
Nishihara T (2004) Efficacy of ozone on survival and permeability of oral microorganisms. Oral Microbiol Immunol 19:240–246 19. Feres M, Haffajee AD, Allard K, Som S, Goodson JM, Socransky
SS (2002) Antibiotic resistance of subgingival species during and after antibiotic therapy. J Clin Periodontol 29:724–735
20. Paoloni M, Di Sante L, Cacchio A, Apuzzo D, Marotta S, Razzano M, Franzini M, Santilli V (2009) Intramuscular oxygen-ozone therapy in the treatment of acute back pain with lumbar disc herniation: a multicenter, randomized, double-blind, clinical trial of active and simulated lumbar paravertebral injection. Spine (Phila Pa 1976) 34:1337–1344
21. Dharap SB, Ghag GS, Kulkarni KP, Venkatesh V (2008) Efficacy and safety of oxum in treatment of the venous ulcer. J Indian Med Assoc 106(326):328–330
22. Lenes D, Deboosere N, Menard-Szczebara F, Jossent J, Alexandre V, Machinal C, Vialette M (2010) Assessment of the removal and inactivation of influenza viruses H5N1 and H1N1 by drinking water treatment. Water Res 44:2473–2486
23. Choi Y, Cho M, Lee Y, Choi J, Yoon J (2007) Inactivation of Bacillus subtilis spores during ozonation in water treatment plant: influence of pre-treatment and consequences for positioning of the ozonation step. Chemosphere 69:675–681
24. Smeets PW, van der Helm AW, Dullemont YJ, Rietveld LC, van Dijk JC, Medema GJ (2006) Inactivation of Escherichia coli by ozone under bench-scale plug flow and full-scale hydraulic conditions. Water Res 40:3239–3248
25. Schwan L, Bamfaste M (1951) Experiences with the use of chlorine gas and ozone in the treatment of root gangrene and dental granuloma. Dtsch Zahnärztl Z 6:248–263
26. Kronenberg O, Lussi A, Ruf S (2009) Preventive effect of ozone on the development of white spot lesions during multibracket appliance therapy. Angle Orthod 79:64–69
27. Baysan A, Lynch E (2007) Clinical reversal of root caries using ozone: 6-month results. Am J Dent 20:203–208
28. Huth KC, Paschos E, Brand K, Hickel R (2005) Effect of ozone on non-cavitated fissure carious lesions in permanent molars. A controlled prospective clinical study. Am J Dent 18:223–228 29. Huth KC, Quirling M, Maier S, Kamereck K, Alkhayer M, Paschos E,
Welsch U, Miethke T, Brand K, Hickel R (2009) Effectiveness of ozone against endodontopathogenic microorganisms in a root canal biofilm model. Int Endod J 42:3–13
30. Yamada K, Yama M, Takaku Y, Kakizawa T, Kimizuka R, Okuda K, Kato T (2010) Antimicrobial activity of super-oxidised water against oral microorganisms. Arch Oral Biol 55:397–400 31. Sharma M, Hudson JB (2008) Ozone gas is an effective and
practical antibacterial agent. Am J Infect Control 36:559–563 32. Hems RS, Gulabivala K, Ng YL, Ready D, Spratt DA (2005) An
in vitro evaluation of the ability of ozone to kill a strain of Enterococcus faecalis. Int Endod J 38:22–29
33. Ozbek SM, Ozbek A, Erdorgan AS (2009) Analysis of Enterococcus faecalis in samples from Turkish patients with primary endodontic infections and failed endodontic treatment by real-time PCR SYBR green method. J Appl Oral Sci 17:370–374
34. Kustarci A, Sumer Z, Altunbas D, Kosum S (2009) Bactericidal effect of KTP laser irradiation against Enterococcus faecalis compared with gaseous ozone: an ex vivo study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107:e73–e79
35. Tew JG, Marshall DR, Burmeister JA, Ranney RR (1985) Relationship between gingival crevicular fluid and serum anti-body titers in young adults with generalized and localized periodontitis. Infect Immun 49:487–493
36. Zeitlinger MA, Sauermann R, Traunmuller F, Georgopoulos A, Muller M, Joukhadar C (2004) Impact of plasma protein binding on antimicrobial activity using time-killing curves. J Antimicrob Chemother 54:876–880
37. Kawamura-Sato K, Wachino J, Kondo T, Ito H, Arakawa Y (2008) Reduction of disinfectant bactericidal activities in clinically isolated Acinetobacter species in the presence of organic material. J Antimicrob Chemother 61:568–576
38. Grenier D, Imbeault S, Plamondon P, Grenier G, Nakayama K, Mayrand D (2001) Role of gingipains in growth of Porphyromonas gingivalis in the presence of human serum albumin. Infect Immun 69:5166–5172
39. Burgassi S, Zanardi I, Travagli V, Montomoli E, Bocci V (2009) How much ozone bactericidal activity is compromised by plasma components? J Appl Microbiol 106:1715–1721
40. Kuboniwa M, Lamont RJ (2010) Subgingival biofilm formation. Periodontol 2000 52:38–52
41. Johansson E, Claesson R, van Dijken JW (2009) Antibacterial effect of ozone on cariogenic bacterial species. J Dent 37:449– 453
42. Muller P, Guggenheim B, Schmidlin PR (2007) Efficacy of gasiform ozone and photodynamic therapy on a multispecies oral biofilm in vitro. Eur J Oral Sci 115:77–80
43. Doroszkiewicz W, Sikorska I, Jankowski S (1994) Studies on the influence of ozone on complement-mediated killing of bacteria. FEMS Immunol Med Microbiol 9:281–285
44. Schenkein HA, Genco RJ (1977) Gingival fluid and serum in periodontal diseases. II. Evidence for cleavage of complement components C3, C3 proactivator (factor B) and C4 in gingival fluid. J Periodontol 48:778–784
45. Potempa M, Potempa J, Kantyka T, Nguyen KA, Wawrzonek K, Manandhar SP, Popadiak K, Riesbeck K, Eick S, Blom AM (2009) Interpain A, a cysteine proteinase from Prevotella intermedia, inhibits complement by degrading complement factor C3. PLoS Pathog 5: e1000316
46. Potempa M, Potempa J, Okroj M, Popadiak K, Eick S, Nguyen KA, Riesbeck K, Blom AM (2008) Binding of complement inhibitor C4b-binding protein contributes to serum resistance of Porphyromonas gingivalis. J Immunol 181:5537–5544
47. Taubman MA, Valverde P, Han X, Kawai T (2005) Immune response: the key to bone resorption in periodontal disease. J Periodontol 76:2033–2041
48. Cochran DL (2008) Inflammation and bone loss in periodontal disease. J Periodontol 79:1569–1576
49. Huth KC, Saugel B, Jakob FM, Cappello C, Quirling M, Paschos E, Ern K, Hickel R, Brand K (2007) Effect of aqueous ozone on the NF-kappaB system. J Dent Res 86:451–456
50. Ducusin RJ, Nishimura M, Sarashina T, Uzuka Y, Tanabe S, Otani M (2003) Phagocytosis of bovine blood and milk polymorphonuclear leukocytes after ozone gas administration in vitro. J Vet Med Sci 65:535–539
51. Huth KC, Jakob FM, Saugel B, Cappello C, Paschos E, Hollweck R, Hickel R, Brand K (2006) Effect of ozone on oral cells compared with established antimicrobials. Eur J Oral Sci 114:435–440