Negative events in childhood predict trajectories of internalizing symptoms up to young adulthood: An 18-year longitudinal study
13
0
0
Texte intégral
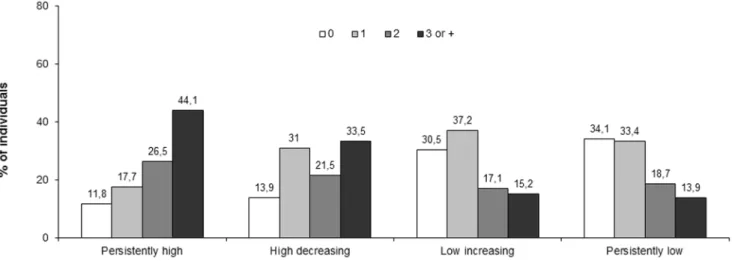
Figure
Documents relatifs
