Ultrasound-guided paravertebral puncture and placement
of catheters in human cadavers: an imaging study
C. Luyet
1, U. Eichenberger
1*, R. Greif
1, A. Vogt
1, Z. Szu¨cs Farkas
2and B. Moriggl
31
Department of Anaesthesiology and Pain Therapy and2Department of Radiology, Inselspital, University Hospital of Bern, and University of Bern, CH-3010 Bern, Switzerland.3Department of Anatomy, Histology,
and Embryology, Innsbruck Medical University, Innsbruck, Austria
*Corresponding author. E-mail: [email protected]
Background. During paravertebral block, the anterolateral limit of the paravertebral space, which consists of the pleura, should preferably not be perforated. Also it is possible that, during the block, the constant superior costotransverse ligament can be missed in the loss-of-resistance technique. We therefore aimed to develop a new technique for an ultrasound-guided puncture of the paravertebral space.
Methods. We performed 20 punctures and catheter placements in 10 human cadavers. A sonographic view showing the pleura and the superior costotransverse ligament was obtained with a slightly oblique scan using a curved array transducer. After inline approach, injection of 10 ml normal saline confirmed the correct position of the needle tip, distended the space, and enabled catheter insertion. The spread of contrast dye injected through the catheters was assessed by CT scans.
Results. The superior costotransverse ligament and the paravertebral space were easy to identify. The needle tip reached the paravertebral space without problems under visualization. In contrast, the introduction of the catheter was difficult. The CT scan revealed a correct para-vertebral spread of contrast in 11 cases. Out of the remaining, one catheter was found in the pleural space, in six cases there was an epidural, and in two cases there was a prevertebral spread of contrast dye.
Conclusions. We successfully developed a technique for an accurate ultrasound-guided punc-ture of the paravertebral space. We also showed that when a catheter is introduced through the needle with the tip lying in the paravertebral space, there is a high probability of catheter misplacement into the epidural, mediastinal, or pleural spaces.
Br J Anaesth 2009; 102: 534–9
Keywords: anaesthetic techniques, regional, paravertebral; analgesic techniques; anatomy, chest wall; monitoring, ultrasound
Accepted for publication: January 16, 2009
The paravertebral block is a regional anaesthetic technique that can be used for analgesia in thoracic,1 – 5 cardiac,6 breast,7 – 9 or upper abdominal surgery10 or for pain therapy.11
Thoracic paravertebral block is performed by injecting a local anaesthetic solution into the paravertebral space, which contains the thoracic nerves, their branches, and the sympathetic trunk.
This space is a wedge-shaped area sandwiched between the head and neck of the ribs. The posterior wall is formed by the superior costotransverse ligament, the anterolateral
wall is the parietal pleura with the endothoracic fascia, and the medial wall is the lateral surface of the vertebral body and disc.12 Also medially, there is communication with the epidural space via the intervertebral foramen. It has been shown that each space communicates inferiorly and superiorly across the head and neck of the ribs.13 – 16Thus by injecting local anaesthetic into the paravertebral space, it results in an analgesia corresponding to a unilateral epi-dural anaesthesia.
Possible advantage of the paravertebral block is that the technique could be safer than the epidural block by
reducing the risk of injury to the thoracic medulla with all its sequelae, the epidural haematoma, epidural infection, and the post-epidural-puncture headache.13
Furthermore, the paravertebral block has fewer side-effects such as urinary retention or hypotension compared with epidural anaesthesia.3
One possibility to reach the paravertebral space is to use the landmark technique with the loss of resistance described first by Eason and Wyatt.13With this technique, the paraver-tebral space is localized blindly according to anatomical landmarks by entering the skin with a needle 2.5 –4 cm lat-erally of the spinous process and penetrating the superior costotransverse ligament by a loss-of-resistance technique. One possible way to achieve a long-lasting analgesia after surgery is to place a catheter in the paravertebral space.3 4 8 9 17 18
In the last few years, there has been a revolution in regional anaesthesia due to the use of ultrasound. Many studies have shown that precise needle placement can be achieved by real-time ultrasound guidance.19 – 25Since the anterolateral delimitation of the paravertebral space con-sists of the pleura, which should preferably not be perfo-rated and the constant superior costotransverse ligament may show a gap between the lateral and the medial
portion and could possibly be missed in the
loss-of-resistance technique18 26 (Fig. 1), we aimed to develop a new technique for an ultrasound-guided punc-ture. We therefore planned this feasibility study on human cadavers consisting of ultrasound-guided puncture of the paravertebral space and placement of a catheter into this space. The accuracy of the catheter placement was tested by consecutive CT control after injection of contrast dye.
Methods
We studied 10 cadavers at the Department of Anatomy, Histology, and Embryology at the Innsbruck Medical
University, Innsbruck, Austria. The cadavers were
embalmed using ethanol and glycerol with a little amount of phenol added. All cadavers were in legal custody of the Department, and Institutional approval for the procedure was obtained.
First, we analysed the paravertebral space and its ana-tomical landmarks on an anatomic model (Figs 1 and 2). The target was to obtain a sonographic view consisting of the pleura and the superior costotransverse ligament between bony landmarks. The best sonographic view of this key structure was obtained with a slightly oblique scan using a curved array transducer (Figs 3 and 4). Depending on the image quality as the main criterion, the degree of obliquity could differ between the sides and the individuals. The superior costotransverse ligament spans between the upper border of a rib’s neck (or the crest of the neck of the rib) and the next higher transverse process (TP). From the level of TH 5 downwards, the neck of the
rib clearly projects above the upper contour of the TP. That is why in the sonogram, the ligament appears to be running from the deep (caudal) to the more superficial (cranial) either from the acoustic shadowing of the rib to that of the next higher TP or between two TPs.
Fig 2On this anatomic model, the strong but narrow superior costotransverse ligament is visible. Behind the ligament on the left and right side, the small dorsal ramus (*) of the thoracic nerve can be seen. On the left side, the larger ventral ramus of the nerve (open arrow), which will form the intercostal nerve more lateral, is visible. The bar shows the slightly oblique axis of the ultrasound probe we chose in order to see the superior costotransverse ligament and pleura.
TP TP
Fig 1This anatomic model shows the superior costotransverse ligament (open arrow) which may show a gap between the lateral and the medial portion, and thus a clear loss of resistance may not be felt in all cases. With the landmark technique, when approaching too far medial, one may enter the costotransverse foramen (small black arrow) or pass the ligament laterally, respectively. The ligament spans between the upper border of a rib’s neck and the next higher TP. From the level of TH 5 downwards, the neck of the rib clearly projects the upper contour of the TP. That is why in the sonogram, the ligament appears to be running from the deep (caudal) to the more superficial (cranial) either from the acoustic shadowing of the rib to that of the next higher TP or between two TPs.
Because we performed an inline puncture to visualize the needle best in relation to the pleura, the needle was guided slightly towards the vertebral column. Despite this direction, the danger of a direct puncture of an interverte-bral foramen (and thus of the epidural space) is prevented by the bony structures of the vertebral column (Fig. 5).
After deciding how to puncture the paravertebral space, two examiners (C.L. and U.E.) experienced in the use of ultrasound for regional anaesthesia performed the new ultrasound-guided approach to the paravertebral spaces at one thoracic level between TH 4 and TH 8 on each side of the vertebral column in each cadaver. Structures were seen
using a portable ultrasound machine (MicromaxTM,
SonoSite Inc., Bothell, WA, USA) and a 2 – 5 MHz curved array transducer. The transducer was first positioned longi-tudinally between two TPs at the level of the future
puncture site. Thereafter, the orientation of the probe was adapted until all mentioned key structures could be undoubtedly identified together with the parietal pleura (the paravertebral space lying between the latter and the superior costotransverse ligament, Fig. 4).
Consecutively, an 18 G Tuohy needle ( peridural catheter set, B. Braun, Melsungen, Germany) was inserted using the described inline approach into the paravertebral space. To dilate the space and to affirm the correct place of the needle tip, 15 ml of 0.9% normal saline was injected through the needle and the dilatation of the paravertebral space was con-firmed by an ultrasound scan. Thereafter, the catheter was inserted through the needle and, as per our routine clinical practice, it was further advanced 5 cm into the paravertebral space and fixed at the skin. If the catheter insertion was not possible, we turned the needle axis a little bit. If the advancement of the catheter was still not possible, we punc-tured again one vertebral level more caudal.
As soon as the catheter was placed and secured between 8 and 15 cm from the skin, we injected 10 ml of diluted contrast dye (300 mg J ml21; Jopamiro, Bracco, Milano, Italy, diluted 1:10 with 0.9% normal saline) through the catheters and the spread of the contrast dye was documen-ted by axial transverse CT scans (5 mm slice) of the entire thoracic column. The spread of the radio-opaque fluid was assessed after termination of the practical part of the study by an independent radiologist (Z.S.F.) who was not other-wise involved in the study.
Results
Ten cadavers were examined (seven males and three females). The cadavers’ mean age at death was 71.2 yr
Fig 5 On a skeleton, the needle direction we chose is demonstrated (larger arrow). The anatomy prevents a direct puncture of the corresponding intervertebral foramen. A direct puncture of the intervertebral foramen could only occur in the case of a very horizontal approach (small arrow).
Fig 3 The curved array transducer is placed in a slightly oblique axis. The needle is inserted inline ( picture taken on a model instead of a cadaver). TP TP R Pleura Costotransverse ligament
Fig 4In this sonogram, the anterior ( pleura) and the posterior (costotransverse ligament) limits of the paravertebral space are visible. R, neck of the rib; TP, transverse process.
(range 50 – 91), mean (SD) body weight 67.9 (6.3) kg,
height 171.4 (6.3) cm, and mean body mass index 24 (range 17 – 33). In total, 20 catheters were placed.
The paravertebral space could be identified and reached without any problem in each cadaver. While injecting saline, the correct position of the needle tip between superior costotransverse ligament and pleura could be veri-fied using real-time ultrasound by visualizing the displace-ment of the pleura in the direction of the lung. The mean shortest distance of the paravertebral space from the skin was 2.7 cm (range 1.7 – 4.31 cm). Because of the slight oblique approach, the mean needle insertion depth was 4.4 cm (range 3.5 – 5.5 cm).
In contrast to the easy puncture of the paravertebral space, the catheter insertion was more difficult. In 30% (6/20) of the instances, the needle axis had to be turned to overcome the difficulty of the catheter placement. In four of the 20 instances, we had to repeat the procedure one level more caudal. In these four instances, the catheters could be inserted at the new level. The mean depth of insertion over the needle tip was 5.3 cm (range from 3.5 to 9.5 cm).
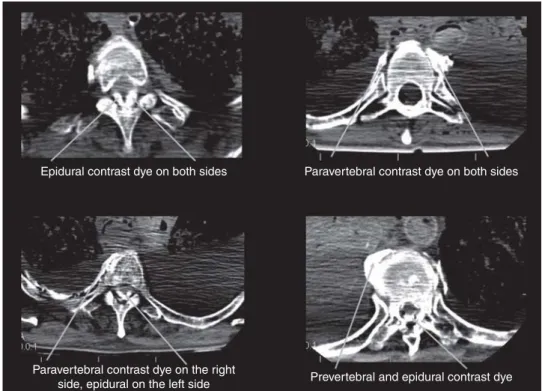
The CT scan control of the spread of contrast was as follows: in one case, the contrast dye was mainly found in the pleural space. In 11 cases, the contrast spread was paravertebral and intercostal across two to six intercostal levels. In two cases, contrast was found in the posterior mediastinum. In six cases, the contrast was found mainly epidural without any contrast in the paravertebral space. The catheter itself could not be identified with certainty. Figure 6 shows different examples of the spread of contrast.
Discussion
With our new sonographic view obtained with a slightly oblique scan, we could display the landmarks of the para-vertebral space including the pleura and the superior costo-transverse ligament. As a result, we could easily introduce the needle through the superior costotransverse ligament and therefore puncture the paravertebral space by using ultrasound guidance. The needle tip position between this ligament and the pleura could be confirmed by real-time sonographic imaging during injection of normal saline through the needle.
The subsequent introduction of a catheter into this space remained technically difficult. In one-third of the cases, needle manipulations had to be executed or another level had to be chosen until the catheter could be advanced. This is similar to the reports of Karmakar and colleagues,12 27 Karmakar and Ho,17and Richardson and Lonnqvist28after needle positioning with the classic landmark technique.
There have been some radiological studies investigating the distribution of contrast dye after paravertebral injec-tion.26 29 30 In contrast to these studies, we for the first time consecutively positioned 20 catheters and evaluated the distribution of contrast dye after injection through the catheter by means of CT.
Surprisingly, in spite of an accurate placement of the needle into the paravertebral space, the distribution of con-trast suggests a migration of the catheters out of the targeted area. In nine cases, the main portion of contrast was found mediastinal (2/20), epidural (6/20), and pleural (1/20). One explanation could be that the catheters migrated along the Epidural contrast dye on both sides Paravertebral contrast dye on both sides
Paravertebral contrast dye on the right
side, epidural on the left side Prevertebral and epidural contrast dye
way of minimal resistance and that the paravertebral space is not a real anatomical compartment as often assumed. It is not clear whether such incorrect catheter positions can be detected clinically by sensory testing as routinely performed. Purcell-Jones and colleagues26 demonstrated 70% epidural spread of contrast even after single-shot injection which resulted in unilateral segmental sensory loss in all cases.
Paravertebral single-shot blocks and catheters are often used in patients with suboptimal coagulation or patients under general anaesthesia instead of epidural catheters because it is thought to be less risky.28 In our view, the single-shot procedure, especially performed under ultra-sound visualization, may be safe even in the high-risk patients. In addition, our findings, similar to other reports,12 26 30 31suggest that the use of paravertebral cath-eter insertion as an alternative to epidural anaesthesia in these patients needs careful evaluation.
There are a few study limitations. The tissue properties of living human subjects could be different from cadavers and therefore limit direct transfer of our data into clinical prac-tice. In order to best visualize the limits of the paravertebral space and to introduce the needle away from the pleura, we have chosen a needle direction pointing towards the ver-tebral column. Even if the bony structure of the verver-tebral column would prevent a direct penetration of the needle into the intervertebral foramen, this does not prevent an easier passage of the catheter from the paravertebral into the epidural space. It is possible that the malposition of the catheters could have been prevented by advancing them ,5 cm. We opted to advance the catheters 5 cm, because it cor-responds to our daily clinical practice and to prevent dislo-cation of catheters during the transfer of cadavers to the CT table. Finally, we have to admit that the chosen design to perform the radiological exam after injection of contrast dye on both sides of the column complicated the interpret-ation of the scans due to possible crossover of contrast dye to the other side or the fact that the epidural contrast dye could not be accurately attributed to one side.
In conclusion, we successfully developed a technique for an ultrasound-guided puncture of the paravertebral space. This new approach allows an easy visualization and accurate puncture of the paravertebral space. On the other hand, when a catheter is introduced through the needle with the tip lying in the paravertebral space, there is a high probability of catheter misplacement into the epidural space, mediastinal, or through the pleura. Whether a more orthogonal needle track or a less deep introduction of the catheter would prevent such phenomena remains to be investigated in a further study. In the meantime, we suggest carefully weighing the risk – benefit ratio whether or not to use thoracic paravertebral catheter techniques.
Acknowledgements
We thank the staff of the Department of Anatomy, Histology, and Embryology of the Medical University of Innsbruck for providing us the cadavers and the locations for the study. Rupert Gstrein (anatomy
technician) helped with the cadavers throughout the study and Bernd Kofler (radiology technician) operated the CT scanner. Special thanks to Jeff Crowder for proofreading the English of this manuscript.
Funding
Only departmental research grants were spent on this research project. The ultrasound device was generously provided by SonoSite Austria, Sittendorf, Austria.
References
1 Richardson J, Sabanathan S, Jones J, Shah RD, Cheema S, Mearns AJ. A prospective, randomized comparison of preoperative and con-tinuous balanced epidural or paravertebral bupivacaine on post-thoracotomy pain, pulmonary function and stress responses. Br J Anaesth 1999; 83: 387–92
2 Perttunen K, Nilsson E, Heinonen J, Hirvisalo EL, Salo JA, Kalso E. Extradural, paravertebral and intercostal nerve blocks for post-thoracotomy pain. Br J Anaesth 1995; 75: 541 – 7
3 Matthews PJ, Govenden V. Comparison of continuous paraverte-bral and extradural infusions of bupivacaine for pain relief after thoracotomy. Br J Anaesth 1989; 62: 204 – 5
4 Lonnqvist PA, MacKenzie J, Soni AK, Conacher ID, Paravertebral blockade. Failure rate and complications. Anaesthesia 1995; 50: 813–5
5 Vogt A, Stieger DS, Theurillat C, Curatolo M. Single-injection thoracic paravertebral block for postoperative pain treatment after thoracoscopic surgery. Br J Anaesth 2005; 95: 816 – 21 6 Ganapathy S, Murkin JM, Boyd DW, Dobkowski W, Morgan J.
Continuous percutaneous paravertebral block for minimally inva-sive cardiac surgery. J Cardiothorac Vasc Anesth 1999; 13: 594 – 6 7 Weltz CR, Greengrass RA, Lyerly HK. Ambulatory surgical
man-agement of breast carcinoma using paravertebral block. Ann Surg 1995; 222: 19 – 26
8 Klein SM, Bergh A, Steele SM, Georgiade GS, Greengrass RA. Thoracic paravertebral block for breast surgery. Anesth Analg 2000; 90: 1402 – 5
9 Pusch F, Freitag H, Weinstabl C, Obwegeser R, Huber E, Wildling E. Single-injection paravertebral block compared to general anaesthesia in breast surgery. Acta Anaesthesiol Scand 1999; 43: 770–4
10 Richardson J, Vowden P, Sabanathan S. Bilateral paravertebral analgesia for major abdominal vascular surgery: a preliminary report. Anaesthesia 1995; 50: 995 – 8
11 Kirvela O, Antila H. Thoracic paravertebral block in chronic post-operative pain. Reg Anesth 1992; 17: 348 – 50
12 Karmakar MK, Chui PT, Joynt GM, Ho AM. Thoracic paraverte-bral block for management of pain associated with multiple frac-tured ribs in patients with concomitant lumbar spinal trauma. Reg Anesth Pain Med 2001; 26: 169 – 73
13 Eason MJ, Wyatt R. Paravertebral thoracic block—a reappraisal. Anaesthesia 1979; 34: 638 – 42
14 Moorthy SS, Dierdorf SF, Yaw PB. Influence of volume on the spread of local anesthetic – methylene blue solution after injection for intercostal block. Anesth Analg 1992; 75: 389 – 91
15 Mowbray A, Wong KK. Low volume intercostal injection. A com-parative study in patients and cadavers. Anaesthesia 1988; 43: 633 – 4
16 Mowbray A, Wong KK, Murray JM, Intercostal catheterisation. An alternative approach to the paravertebral space. Anaesthesia 1987; 42: 958 – 61
17 Karmakar MK, Ho AM. Acute pain management of patients with multiple fractured ribs. J Trauma 2003; 54: 615 – 25
18 Boezaart AP, Raw RM. Continuous thoracic paravertebral block for major breast surgery. Reg Anesth Pain Med 2006; 31: 470 – 6 19 Eichenberger U, Greher M, Kirchmair L, Curatolo M, Moriggl B.
Ultrasound-guided blocks of the ilioinguinal and iliohypogastric nerve: accuracy of a selective new technique confirmed by ana-tomical dissection. Br J Anaesth 2006; 97: 238 – 43
20 Greher M, Kirchmair L, Enna B, et al. Ultrasound-guided lumbar facet nerve block: accuracy of a new technique confirmed by computed tomography. Anesthesiology 2004; 101: 1195 – 200 21 Kirchmair L, Entner T, Kapral S, Mitterschiffthaler G. Ultrasound
guidance for the psoas compartment block: an imaging study. Anesth Analg 2002; 94: 706 – 10, table of contents
22 Lo N, Brull R, Perlas A, et al. Evolution of ultrasound guided axil-lary brachial plexus blockade: retrospective analysis of 662 blocks: (Evolution du bloc du plexus brachial par approche axil-laire sous echoguidage: une analyse retrospective de 662 blocs). Can J Anaesth 2008; 55: 408 – 13
23 Chan VW, Perlas A, McCartney CJ, Brull R, Xu D, Abbas S. Ultrasound guidance improves success rate of axillary brachial plexus block. Can J Anaesth 2007; 54: 176 – 82
24 Marhofer P, Chan VW. Ultrasound-guided regional anesthesia: current concepts and future trends. Anesth Analg 2007; 104: 1265–9, tables of contents
25 Willschke H, Bosenberg A, Marhofer P, et al. Epidural catheter placement in neonates: sonoanatomy and feasibility of ultrasono-graphic guidance in term and preterm neonates. Reg Anesth Pain Med 2007; 32: 34 – 40
26 Purcell-Jones G, Pither CE, Justins DM. Paravertebral somatic nerve block: a clinical, radiographic, and computed tomo-graphic study in chronic pain patients. Anesth Analg 1989; 68: 32 – 9
27 Karmakar MK, Critchley LA, Ho AM, Gin T, Lee TW, Yim AP. Continuous thoracic paravertebral infusion of bupivacaine for pain management in patients with multiple fractured ribs. Chest 2003; 123: 424 – 31
28 Richardson J, Lonnqvist PA. Thoracic paravertebral block. Br J Anaesth 1998; 81: 230 – 8
29 Karmakar MK, Kwok WH, Kew J. Thoracic paravertebral block: radiological evidence of contralateral spread anterior to the ver-tebral bodies. Br J Anaesth 2000; 84: 263 – 5
30 Conacher ID, Kokri M. Postoperative paravertebral blocks for thoracic surgery. A radiological appraisal. Br J Anaesth 1987; 59: 155 – 61
31 Lekhak B, Bartley C, Conacher ID, Nouraei SM. Total spinal anaesthesia in association with insertion of a paravertebral cath-eter. Br J Anaesth 2001; 86: 280 – 2