HAL Id: hal-02992331
https://hal-amu.archives-ouvertes.fr/hal-02992331
Submitted on 6 Nov 2020HAL is a multi-disciplinary open access archive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come from teaching and research institutions in France or abroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, est destinée au dépôt et à la diffusion de documents scientifiques de niveau recherche, publiés ou non, émanant des établissements d’enseignement et de recherche français ou étrangers, des laboratoires publics ou privés.
Improved Cervical Cord Lesion Detection with
3D-MP2RAGE Sequence in Patients with Multiple
Sclerosis
S. Demortière, P. Lehmann, Jean Pelletier, Bertrand Audoin, Virginie Callot
To cite this version:
S. Demortière, P. Lehmann, Jean Pelletier, Bertrand Audoin, Virginie Callot. Improved Cervical Cord Lesion Detection with 3D-MP2RAGE Sequence in Patients with Multiple Sclerosis. Amer-ican Journal of Neuroradiology, AmerAmer-ican Society of Neuroradiology, 2020, 41 (6), pp.1131-1134. �10.3174/ajnr.A6567�. �hal-02992331�
Improved cervical cord lesion detection with 3D MP2RAGE sequence
in patients with multiple sclerosis
Sarah Demortière 1,2, Pierre Lehmann 2,3, Jean Pelletier 1,2, Bertrand Audoin 1,2 and Virginie Callot 1,4,*
1 APHM, Hôpital Universitaire Timone, CEMEREM, Marseille, France
2 Department of Neurology, CHU Timone, AP-HM, Marseille, France 3 Department of Neuroradiology, CHU Timone, AP-HM, Marseille, France 4 Aix-Marseille Univ, CNRS, CRMBM, Marseille, France
* Corresponding author: Virginie CALLOT
CRMBM-CEMEREM, UMR 7339, CNRS - Aix-Marseille Université, Faculté de Médecine 27, bd Jean Moulin, 13385 Marseille Cedex 5, France.
E-mail : [email protected] Tel : +33 4 91 38 84 65
Grant support :
This work was performed within a laboratory member of France Life Imaging network (grant ANR-11-INBS-0006) and supported by ARSEP (Fondation pour l'Aide à la Recherche sur la Sclérose En Plaques) and CNRS (Centre National de la Recherche Scientifique).
Abstract
Spinal cord lesions have a real diagnostic and prognostic role in multiple sclerosis. Thus, optimizing their detection on MRI has become a central issue with direct therapeutic impact. In this study, we compared the 3D MP2RAGE sequence to the conventional MAGNIMS set for cervical cord lesion detection in 28 patients with multiple sclerosis. 3D MP2RAGE allowed for better detection of cervical lesions (+62%) in this population, with better confidence, thanks to optimized contrast and high spatial resolution.
Introduction
Since the last revision of the Magnetic Resonance Imaging in Multiple Sclerosis (MAGNIMS) guidelines1 and McDonald’s criteria of 20172, all spinal cord (SC) lesions must be counted to increase the sensitivity and specificity of multiple sclerosis (MS) diagnosis3. In this context, standardized acquisition protocols have been proposed1. For SC MRI, at least
two sagittal sequences among T2-weighted (T2-w), STIR, double inversion recovery, T1-w with gadolinium injection and/or T2-w axial acquisitions1 are recommended. Nonetheless, different sequences are often necessary because of motion and flux artifacts4, which is time-consuming.
The Magnetization Prepared 2 Rapid Acquisition Gradient Echoes (MP2RAGE) sequence5 has been shown to significantly improve the detection of cerebral lesions that are difficult to visualize on conventional sequences, such as cortical lesions6. This T1-w MRI sequence, which creates a composite image limiting field inhomogeneity bias while providing a quantitative T1 map, has recently been optimized for SC7 but not yet evaluated in the context of MS.
The aim of this study was to compare the MP2RAGE sequence to the conventional set of routine sequences for detecting SC lesions in patients with MS.
Materials and methods
PatientsThis retrospective study, approved by the local ethics committee with written informed consent, included 28 patients with MS from January 2017 to January 2019. Inclusion criteria were diagnosis of MS according to the revised McDonald criteria2, age>18 years, clinical
Image acquisition
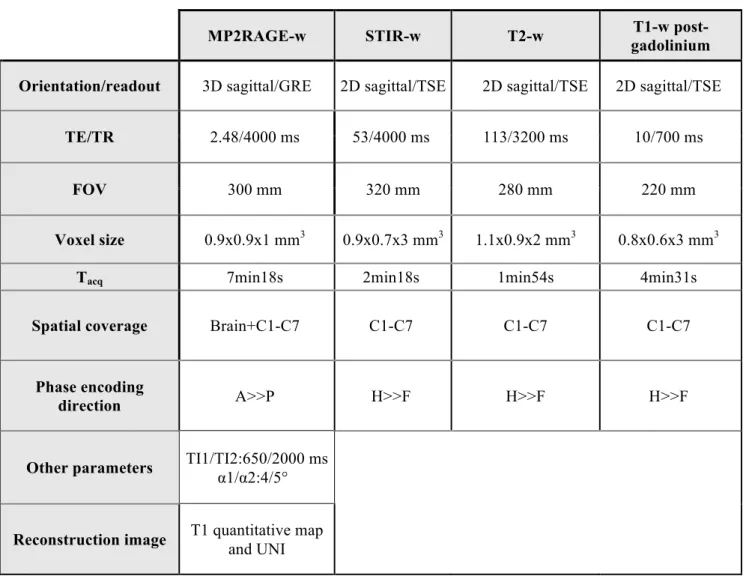
Sequences were acquired on a 3T system (MAGNETOM Verio, Siemens Healthineers, Erlangen, Germany) during the same examination. The protocol was as follows (see Table 1 for MR parameters):
- one sagittal 3D MP2RAGE sequence, providing two contrasted images, Tinv1 and Tinv2, from which a uniform image (UNI) free of B1 inhomogeneities and a T1 map were derived5, and
- a conventional set with sagittal 2D T2-w, STIR-w and T1-w post-gadolinium sequences, with axial 2D T2*-w MRI for confirmation of suspicious lesions on a sagittal set
Lesion detection and scoring confidence
The cervical SC from C1-C7 was evaluated. Two operators, a senior neuroradiologist and neurologist, who were blinded to patient data, read the results of the conventional set and 3D MP2RAGE sequence (T1 map and UNI image). Identification took place during a consensus session8, on a high-resolution monitor, by using syngo.via Siemens image analysis software. MS lesions were detected based on hyperintensity on T2-w, STIR, MP2RAGE T1 map, and T1-w post-gadolinium images in case of inflammatory lesions or hypointensity seen on MP2RAGE uniform images, as compared with normal cord signals. The lesion had to be visible on at least two slices in a row for the millimetric MP2RAGE sequence. According to the MAGNIMS criteria, a lesion was validated if visible on at least two sequences of the conventional set. Lesion detection was reevaluated (reproducibility assessment) 3 weeks later, to minimize recall bias.
Confidence in detection was defined during the consensus session by use of a qualitative scale9: 0, no lesion detected; 1, low detection confidence; 2, moderate-to-high detection confidence; and 3, very high detection confidence.
Statistical analysis
Wilcoxon tests (JMP9, SAS Institute, Cary, USA) were used to compare the number of detected lesions between conventional and MP2RAGE datasets, as well as the reader’s confidence between sequences. P < 0.05 was considered statistically significant.
Results
Demographic and clinical characteristics
We included 28 patients with MS (19 women; median age 34.5 years [interquartile range 28-41]; 23 had relapsing-remitting MS, 4 secondary-progressive MS and 1 primary-progressive MS. The mean Expanded Disability Status Scale score was 1.5±1.4 (range 0-6.5). The median disease duration was 4.8 years [interquartile range 1.7-10.1].
Spinal cord lesions
In total, 27 patients had at least 1 identifiable SC lesion and 2 had an active enhancing lesion. A total of 117 lesions were detected. All lesions identified during the first image-analysis session were found during the second session (100% reproducibility). MP2RAGE significantly revealed more lesions than the conventional set (p < 0.0001) (Figure 1). All lesions seen by the conventional sagittal set were detected in MP2RAGE.
Conversely, 13 lesions (7 patients) were detected only by MP2RAGE. These lesions had an average [min/max] diameter of 2.6 [1.9/4.1] mm. They all fulfilled the characteristics of MS lesions10 in terms of size and location (54% posterior, 31% lateral and 15% anterior), and
their presence was carefully double-checked in the axial/coronal plane. The image quality of the conventional set for the corresponding slices was carefully re-evaluated and was satisfactory. Among these 7 patients, 3 had no visible lesions at all on conventional set detection (supplementary table 1 and Figure 2).
Detection confidence
Mean reading confidence was significantly higher with MP2RAGE than STIR (2.1±0.7 vs 1.5±1.2, p = 0.0011) and T2 (2.1±0.7 vs 0.7±0.9, p < 0.0001) sequences. Confidence did not differ between lesions detected by MP2RAGE alone and those seen jointly by MP2RAGE and the conventional set (2.0±0.6 vs 2.2±0.8, p = 0.11).
Discussion
The present study highlights for the first time in MS that the 3D MP2RAGE method is able to detect cervical cord lesions with higher confidence and higher sensitivity than the recommended conventional MAGNIMS set. Given the essential diagnostic and prognostic significance of SC lesions in MS, these results could have some critical added value for clinical practice, as previously demonstrated using phase-sensitive inversion recovery or double inversion recovery contrast9-11 .
In this work, 3D MP2RAGE detected significantly more lesions than did STIR, T2-w and MAGNIMS set sequences. Importantly, it also allowed for detecting lesions in patients classified as not having cord lesions with the conventional set (11%). Of note, the validation of these undetected lesions was the subject of consensus between two experienced operators, repeated once with blinding to the previous assessment. Furthermore, the detection confidence for all the lesions visualized by MP2RAGE alone (2.0±0.6, n=13 lesions) was as high as for those visualized by both MP2RAGE and the conventional set, which consolidates
our findings. Finally, the characteristics of these lesions were typical for MS10 showing, for
the first time in the cord, similar results than previously reported in the brain12-14. Recent study
also demonstrated good correlation between cerebral lesions detected with MP2RAGE and histological findings6, however such data were not available in the present study and similar
work remains to be done.
The present study has some additional limitations. First, the sample size was small and did not include patients with clinical isolated syndrome, for which it will be necessary to assess the potential value of MP2RAGE diagnosis. Second, the respective contrast-to-noise ratios of the different sequences were not compared because of different spatial resolutions and partial volume effects. According to the present study design, we cannot exclude that the better sensitivity of the MP2RAGE is mostly related to its 3D isotropic nature rather than its better ability for visualizing lesions whatever their size. Indeed, some authors reported a gain in sensitivity in 3D sequences15,16 from 28% to 65% for cervical lesion detection9,11,17. Comparison between 3D MP2RAGE, 3D STIR and 3D T2-WI is left for future specific studies. Concerning the 3 patients for whom no lesions were detected by the conventional set, missed lesions were mainly due to their small size with regard to sequence spatial resolutions. However, 8/13 lesions detected only with the MP2RAGE sequence exceeded the spatial resolution of the conventional set, which suggests that the better sensitivity of MP2RAGE may be related more to its better contrast than its 3D isotropic resolution.
Finally, the MP2RAGE acquisition time (7 min) may seem relatively long as compared with the 2D individual sequences. However, the volume acquired here covered the whole brain and the entire cervical SC with isotropic sub-millimetric resolution. This offers promising opportunities for global assessment of the upper part of the central nervous system (brain and upper cervical cord). Brain evaluation was beyond the scope of this study. Finally, a
compressed-sensing version of the sequence is now proposed18, which may further improve the added clinical value of the MP2RAGE sequence.
Further assessments and multi-centric studies must now be promoted to improve lesion detection capabilities, clinical evaluation and bring additional proofs of specificity.
Conclusion
In this study, an optimized 3D MP2RAGE sequence was demonstrated to allow a significant gain in the detection of MS cervical lesions (including in patients otherwise presenting no lesions on conventional MRI), with high reader confidence assessment, as compared to conventional set. This MP2RAGE protocol, allowing brain and cervical cord coverage in 7 min, could be promising to improve clinical practice. Future study using larger samples are necessary to confirm these preliminary results.
Acknowledgements
The authors thank V.Gimenez, L.Pini, C.Costes and MP.Ranjeva for study logistics; A.Rico for patient recruitment; A.Massire, JP.Ranjeva and A.Maarouf for helpful discussions; and T.Kober (Siemens Healthcare) for MP2RAGE sequence provision.
This work was performed within a laboratory member of France Life Imaging network (grant ANR-11-INBS-0006) and was supported by the ARSEP Fundation (Fondation pour l’Aide à la recherche sur la Sclérose en Plaques) and CNRS (Centre National de la Recherche Scientifique).
References
1. Filippi.M, Rocca.MA, Ciccarelli.O, et al. MRI criteria for the diagnosis of multiple-sclerosis: MAGNIMS consensus guidelines. Lancet.Neurol2016;15:292–303.
2. Thompson.AJ, Banwell.BL, Barkhof.F, et al. Diagnosis of multiple -clerosis: 2017 revisions of the McDonald criteria. Lancet.Neurol2018;17:162–73.
3. Filippi.M, Preziosa.P, Meani.A, et al. Prediction of a multiple-sclerosis diagnosis in patients with clinically isolated syndrome using the 2016 MAGNIMS and 2010 McDonald criteria: a
retrospective study. Lancet.Neurol2018;17:133–42.
4. Vargas.MI, Delavelle.J, Kohler.R, et al. Brain and spine MRI artifacts at 3Tesla. J.Neuroradiol.J.Neuroradiol2009;36:74–81.
5. Marques.JP, Kober.T, Krueger.G, et al. MP2RAGE, a self bias-field corrected sequence for improved segmentation and T1-mapping at high field. NeuroImage2010;49:1271–81.
6. Beck.ES, Sati.P, Sethi.V, et al. Improved Visualization of Cortical Lesions in Multiple-Sclerosis Using 7TMP2RAGE. Am.J.Neuroradiol2018;39:459–66.
7. Rasoanandrianina.H, Massire.A, Taso.M, et al. Regional T1 mapping of the whole cervical spinal cord using an optimized MP2RAGE sequence. NMR.Biomed2019;32:e4142.
8. Poonawalla.AH, Hou.P, Nelson.FA, et al. Cervical Spinal Cord Lesions in Multiple-Sclerosis: T1-weighted Inversion-Recovery MR Imaging with Phase-Sensitive Reconstruction.
Radiology2008;246:258–64.
9. Fechner.A, Savatovsky.J, El Methni.J, et al. A 3T Phase-Sensitive Inversion Recovery MRI Sequence Improves Detection of Cervical Spinal-Cord Lesions and Shows Active Lesions in Patients with Multiple-Sclerosis. AJNR.Am.J.Neuroradiol2019;40:370–5.
10. Moccia.M, Ruggieri.S, Ianniello.A, et al. Advances in spinal-cord imaging in multiple-sclerosis. Ther Adv Neurol Disord 2019;12:1756286419840593.
11. Mirafzal.S, Goujon.A, Deschamps.R, et al. 3D PSIR MRI at 3Tesla improves detection of spinal-cord lesions in multiple-sclerosis. J.Neurol2020;267:406–14.
12. Kober.T, Granziera.C, Ribes.D, et al. MP2RAGE multiple-sclerosis magnetic resonance imaging at 3 T. Invest.Radiol2012;47:346–52.
13. Fartaria.MJ, Bonnier.G, Roche.A, et al. Automated detection of white matter and cortical lesions in early stages of multiple-sclerosis. J.Magn.Reson.ImagingJMRI2016;43:1445–54. 14. Fartaria.MJ, Sati.P, Todea.A, et al. Automated Detection and Segmentation of Multiple--Sclerosis Lesions Using Ultra-High-Field MP2RAGE. InvestRadiol2019;54:356–64.
15. Nayak.NB, Salah.R, Huang.JC, et al. A comparison of sagittal short T1 inversion recovery and T2-weighted FSE sequences for detection of multiple-sclerosis spinal cord lesions.
Acta.Neurol.Scand2014;129:198–203.
16. Chong.AL, Chandra.RV, Chuah.KC, et al. Proton Density MRI Increases Detection of Cervical Spinal-Cord Multiple-Sclerosis Lesions Compared with T2-Weighted Fast Spin-Echo. Am.J.Neuroradiol2016;37:180–4.
17. Riederer.I, Karampinos.DC, Settles.M, et al. Double inversion recovery sequence of the cervical spinal-cord in multiple sclerosis and related inflammatory diseases.
AJNR.Am.J.Neuroradiol2015;36:219–25.
18. Mussard.E, Hilbert.T, Meuli.R,et al. Accelerated MP2RAGE Imaging Using Sparse Iterative Reconstruction. Proceeding of the 24th ISMRM meeting,2016, p.4216
Tables and figures
Table 1. Main sequence parameters.
MP2RAGE-w STIR-w T2-w T1-w
post-gadolinium Orientation/readout 3D sagittal/GRE 2D sagittal/TSE 2D sagittal/TSE 2D sagittal/TSE
TE/TR 2.48/4000 ms 53/4000 ms 113/3200 ms 10/700 ms
FOV 300 mm 320 mm 280 mm 220 mm
Voxel size 0.9x0.9x1 mm3 0.9x0.7x3 mm3 1.1x0.9x2 mm3 0.8x0.6x3 mm3
Tacq 7min18s 2min18s 1min54s 4min31s
Spatial coverage Brain+C1-C7 C1-C7 C1-C7 C1-C7
Phase encoding
direction A>>P H>>F H>>F H>>F
Other parameters TI1/TI2:650/2000 ms α1/α2:4/5°
Reconstruction image T1 quantitative map and UNI
Abbreviations: -w: -weighted; GRE: gradient recalled echo; TSE: turbo spin echo; TE: echo time; TR: repetition time; FOV: field of view; Tacq: acquisition time; TI: inversion time; A: anterior; P:
Supplementary table. Number of lesions detected, by patient and MR sequence
Patients
MR sequences
MP2RAGE MAGNIMS * STIR T2-w T1-w
post-gadolinium Patient 1 7 5 6 5 0 Patient 2 6 4 5 3 1 Patient 3 7 7 7 6 0 Patient 4 4 2 3 0 0 Patient 5 6 6 6 4 0 Patient 6 9 7 9 5 0 Patient 7 4 3 3 3 0 Patient 8 1 1 1 0 0 Patient 9 1 1 0 1 0 Patient 10 5 3 4 3 0 Patient 11 1 1 1 1 0 Patient 12 11 7 9 4 0 Patient 13 7 3 3 3 0 Patient 14 7 1 0 0 0 Patient 15 5 4 4 4 0 Patient 16 6 4 5 2 0 Patient 17 2 1 1 1 0 Patient 18 2 0 0 0 0 Patient 19 0 0 0 0 0 Patient 20 2 1 1 1 NA Patient 21 2 2 1 2 0 Patient 22 1 0 0 0 NA Patient 23 3 2 2 2 0 Patient 24 7 3 4 0 0 Patient 25 5 3 4 2 1 Patient 26 4 1 3 0 0 Patient 27 1 0 0 0 0 Patient 28 1 1 1 0 0
NA: not available. *: according to the MAGNIMS criteria, a lesion was validated if visible on at least two sequences of the conventional set.