The 825C/T polymorphism of the G‐protein subunit β3 does not influence blood pressure and renal function in kidney transplant recipients
4
0
0
Texte intégral
(2) 1664. R. P. Wu¨ thrich et al.. recorded at 3-month intervals for the first year after transplantation.. Genotyping of Gb3 polymorphism The DNA was isolated from whole blood using the QIAampB blood midi kit (Qiagen AG, Basel, Switzerland ). The DNA was amplified by polymerase chain reaction as originally described by Siffert et al. [3]. Ten microlitres of the reaction was digested with 2.5 U of BseDI overnight at 55°C in a total volume of 20 ml. The digested reaction volume was then separated on a 2.5% Nusieve agarose gel. After staining with 0.5 mg/ml ethidium bromide the gel was visualized under UV illumination and photographed. The 268-bp fragment corresponds to the TT genotype (no restriction), the CC genotype generates bands of 116 and 152 bp (complete restriction). The heterozygous CT genotype is characterized by bands at 116, 152 and 268 bp.. Statistical analysis Data are given as mean and standard deviation (SD). Frequencies of the alleles and genotypes were counted and were compared by the use of the x2 test with the values predicted under the assumption of a Hardy– Weinberg equilibrium in the samples. Genotype and allele frequencies were compared between normal blood donors and renal transplant recipients also using the x2 statistics.. Results First we analysed the genotype distribution and the Gb3 allele frequencies in normal healthy blood donors (n=163) and compared the values to the renal transplant recipients (n=216). Table 1 demonstrates that there was a slight increase in the percentage of transplant recipients with the TT genotype (4.5% increase) and also a slightly higher T allele frequency (5% increase) which was not statistically significant. Genotype frequencies complied with the Hardy– Weinberg equilibrium in both populations. When stratifying the genotype and allele frequencies according to the original renal disease, we found an increased percentage of the TT genotype and T allele in patients with glomerular diseases ( Table 2). In the 27 patients with the TT genotype, 48% had glomerulonephritis (GN ) as the underlying disease (including chronic GN, focal and segmental glomerulosclerosis, membranoproliferative GN, and IgA nephropathy).. This percentage amounted only to 29% for the CT (n=94) and 27% for the CC genotype (n=95) (P= 0.034). The increased frequency of the T allele in these patients may therefore indicate a possible role in the development of glomerular diseases. We then analysed basic patient characteristics according to the different genotypes. Table 3 shows that the Gb3 genotype was not significantly associated with age, sex, height, weight, and body mass index. We also examined whether Gb3 had an influence on BP and use of BP medication in the renal transplant population. Table 4 demonstrates that there was no significant difference in the systolic, diastolic and mean BP after renal transplantation. Twelve months after transplantation the percentage of patients needing BP medication was similar, amounting to 86% for CC, 89% for CT and 74% for TT genotypes (P=n.s.). Table 4 also demonstrates that the mean number of BP medication needed to control post-transplantation hypertension was similar for the three genotypes. Thus, the Gb3 genotype does not appear to promote hypertension in renal transplant recipients. Analysing the renal function within the first year after transplantation we also found no association between serum creatinine and the different Gb3 genotypes. Table 5 shows that renal function was excellent in all three groups. Values tended to be even slightly lower for the TT genotype, but this was not statistically significant. We also examined whether the immunosuppressive regimen was different in the three genotypes, but we could not find any difference (data not shown).. Discussion In several studies it has been shown that the T allele of Gb3 is associated with the occurrence of hypertension [3–5]. It has been postulated that the truncated Gb3-s protein, which results from the replacement of C by T at position 825, could be causing hypertension via enhanced signalling through pertussis-sensitive G proteins [3]. It has also been suggested that the increased G protein signalling is linked to increased Na+/H+ exchange, although the relation between G protein signalling, increased Na+/H+ and the development of hypertension has not been defined precisely. Hypertension is a frequent problem after renal transplantation [6,7]. Close to 90% of our patients were. Table 1. Genotype and allele frequencies of the Gb3 C825T alleles Genotype. Normal population (n=163) Renal-transplant patients (n=216). Allele frequency. CC. CT. TT. C. T. 80 (49.1%) 95 (44.0%). 70 (42.9%) 94 (43.5%). 13 (8%) 27 (12.5%). 0.71 0.66. 0.29 0.34. Overall genotype and allele frequencies in both populations are reported. Populations were compared with the x2 test and were not significantly different (x2=2.332, 2 df, P=0.3116)..
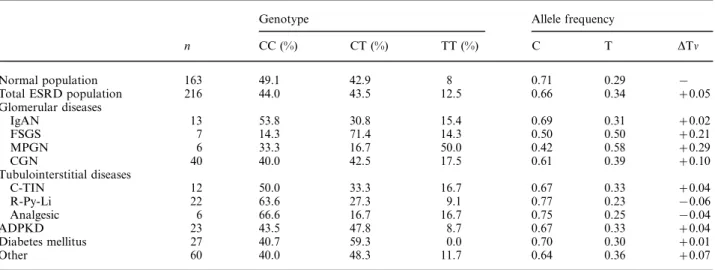
(3) Polymorphism of the G-protein subunit b3 and blood pressure. 1665. Table 2. Subgroup analysis of the C825T polymorphism in the renal transplant population according to original renal disease (%) Genotype. Normal population Total ESRD population Glomerular diseases IgAN FSGS MPGN CGN Tubulointerstitial diseases C-TIN R-Py-Li Analgesic ADPKD Diabetes mellitus Other. Allele frequency. n. CC (%). CT (%). TT (%). C. T. DTn. 163 216. 49.1 44.0. 42.9 43.5. 8 12.5. 0.71 0.66. 0.29 0.34. − +0.05. 13 7 6 40. 53.8 14.3 33.3 40.0. 30.8 71.4 16.7 42.5. 15.4 14.3 50.0 17.5. 0.69 0.50 0.42 0.61. 0.31 0.50 0.58 0.39. +0.02 +0.21 +0.29 +0.10. 12 22 6 23 27 60. 50.0 63.6 66.6 43.5 40.7 40.0. 33.3 27.3 16.7 47.8 59.3 48.3. 16.7 9.1 16.7 8.7 0.0 11.7. 0.67 0.77 0.75 0.67 0.70 0.64. 0.33 0.23 0.25 0.33 0.30 0.36. +0.04 −0.06 −0.04 +0.04 +0.01 +0.07. Subgroup analysis for C825T polymorphism is reported according to original renal disease. ADPKD, autosomal dominant polycystic kidney disease; CGN, chronic glomerulonephritis; C-TIN, chronic tubulointerstitial nephritis; ESRD, end-stage renal disease; FSGS, focal and segmental glomerulosclerosis; IgAN, IgA nephropathy; MPGN, membranoproliferative glomerulonephritis; R-Py-Li, interstitial disease due to reflux, pyelonephritis, and lithiasis. Differences in allele frequencies compared with the normal population (DTn) are also indicated. Table 3. Correlation between Gb3 genotype and age, sex, and BMI Genotype. CC. CT. TT. Age Sex (F:M ) Height (cm) Weight (kg) BMI (kg/m2). 44.2±13.4 40:54 (42.6% F ) 169.3±9.1 71.2±13.0 24.9±4.5. 45.0±14.0 27:66 (29% F ) 171.1±10.1 71.2±12.2 24.3±3.2. 43.6±12.4 12:15 (44.4% F ) 168.9±9.5 72.5±10.3 25.4±2.7. Age, sex, height, weight and body mass index (BMI ) according to Gb3 genotype. The latter was calculated as weight/(height)2 (kg/m2). Groups are not different. A non-significant lower percentage of females was noted in the CT group (P=0.1096). Table 4. Influence of Gb3 genotype on post-transplantation BP and use of BP medication. Table 5. Lack of influence of Gb3 genotype on post-transplantation renal function. Genotype. Genotype. CC. CT. TT. 3-month values 6-month values 9-month values 12-month values. 137±42 139±40 140±36 141±37. 124±27 125±29 130±29 135±45. 123±29 123±23 132±33 131±27. CC. 6-month values SBP 133.6±20.6 DBP 79.3±11.1 MBP 98.5±13.2 BP med (n) 1.9±1.0 12-month values SBP 135.8±17.4 DBP 82.7±10.8 MBP 100.4±11.5 BP med (n) 1.8±1.1. CT. TT. 138.1±19.1 79.4±9.2 100.3±10.1 1.6±1.0. 131.6±18.4 78.5±9.6 97.4±10.8 1.7±1.1. 136.4±21.1 80.8±12.7 99.4±13.5 1.7±1.0. 138.6±22.2 81.7±11.0 100.7±12.9 1.6±1.2. Six-monthly BP measurements (mmHg) and the number of BP medications were averaged for the Gb3 CC, CT, and TT genotypes. Data represent mean±SD. SBP, systolic BP; DBP, diastolic BP; MBP, mean BP. There was no significant difference in BP and medication use between the three genotypes.. hypertensive after transplantation, needing one ore more drugs to control BP. In our study we fail to demonstrate an effect of the Gb3 T allele on BP after transplantation, and the T allele did also not influence the need for BP medication in our transplant population. This would suggest that enhanced G-protein. As a measure of the renal transplant function, serum creatinine levels (mmol/l; mean±SD) are reported after 3, 6, 9 and 12 months.. signalling does not play a major role in the pathogenesis of hypertension in the post-transplant setting. Hypertension after renal transplantation is frequently multifactorial, and various other factors such as the volume status or the immunosuppressive regimen (steroids, calcineurin antagonists) could play an overriding role. There are other studies that have also failed to demonstrate a significant role of the T allele in human hypertension, due perhaps to differences in the genetic background or due to age-specific effects [8,9]. In fact the effect of Gb3 might be restricted to older patients with low-renin essential hypertension as pointed out.
(4) 1666. by Schunkert et al. [10]. While confirming the association of Gb3 and hypertension, Beige et al. [5] also failed to demonstrate an effect of the T allele on the level of systolic and diastolic BP and the number of BP medications in patients with essential hypertension. It therefore appears that Gb3 does not influence the level of hypertension or the use of BP medication in patients with already established hypertension. We also show that the T allele of the Gb3 protein does not have a negative impact on early renal function. Serum creatinine levels were comparable for the CC, CT and TT genotypes in the first year after transplantation. This is in agreement with a recently published study examining the Gb3 polymorphism in kidney donors and recipients, although follow-up was shorter in our study [11]. Interestingly, in that study the donor but not the recipient T allele was found to influence graft survival, suggesting that altered signalling via pertussis-sensitive G proteins could promote the development of chronic rejection. Our data demonstrate that the overall genotype distribution of the 825C/T polymorphism is not significantly altered in a population of renal transplant recipients when compared with a population of normal blood donors. In the subgroup of patients with glomerular diseases, however, the T allele was significantly enriched, and GN was the most frequent underlying renal disease in patients with the TT genotype. This finding has also been documented by Beige et al. [11]. The pathophysiological significance of this association remains to be defined. One pathophysiological link could involve increased chemotaxis for individuals carrying the T allele, as a recent study has demonstrated enhanced fMLP-stimulated chemotactic activity for neutrophils with the T allele [12]. Furthermore, enhanced chemotaxis of human neutrophils in response to interleukin-8 was also found in individuals with the CT or TT genotype [13]. At present there is only limited information available regarding the association of the T allele with renal disease. No significant association was found with diabetic nephropathy in type I diabetes mellitus [14], whereas the T allele frequency was found to be elevated in type II diabetics on dialysis [15]. Clearly, the impact of the Gb3 polymorphism on the development of various types of renal disease needs to be investigated in larger and more homogeneous population samples. In summary, we failed to demonstrate a significant association of the 825C/T polymorphism of Gb3 with the occurrence of renal disease in a large population of renal patients with status post-transplantation. Furthermore, we found no influence of the T allele on. R. P. Wu¨ thrich et al.. BP and BP medication as well as early (<1-year) renal function. Long-term follow-up of these patients is planned, to examine whether the recipient T allele plays a role in BP control and in the development of chronic rejection. Acknowledgements. RPW is the recipient of a SCORE-A career development award by the Swiss National Science Foundation (grant no. 32–38821.93). We thank V. Anukege and R. Russi for valuable technical assistance.. References 1. Siffert W, Rosskopf D, Moritz A et al. Enhanced G protein activation in immortalized lymphoblasts from patients with essential hypertension. J Clin Invest 1995; 96: 759–766 2. Rosskopf D, Fromter E, Siffert W. Hypertensive sodium-proton exchanger phenotype persists in immortalized lymphoblasts from essential hypertensive patients. A cell culture model for human hypertension. J Clin Invest 1993; 92: 2553–2559 3. Siffert W, Rosskopf D, Siffert G et al. Association of a human G-protein b3 subunit variant with hypertension. Nature Genet 1998; 18: 45–48 4. Benjafield AV, Jeyasingam CL, Nyholt DR, Griffiths LR, Morris BJ. G-protein b3 subunit gene (GNB3) variant in causation of essential hypertension. Hypertension 1998; 32: 1094–1097 5. Beige J, Hohenbleicher H, Distler A, Sharma AM. G-Protein b3 subunit C825T variant and ambulatory blood pressure in essential hypertension. Hypertension 1999; 33: 1049–1051 6. Luke RG. Pathophysiology and treatment of posttransplant hypertension. J Am Soc Nephrol 1991; 2: S37–S44 7. Luke RG. Mechanism of cyclosporine-induced hypertension. Am J Hypertens 1991; 4: 468–471 8. Kato N, Sugiyama T, Morita H et al. G protein b3 subunit variant and essential hypertension in Japanese. Hypertension 1998; 32: 935–938 9. Brand E, Herrmann SM, Nicaud V et al. The 825C/T polymorphism of the G-protein subunit b3 is not related to hypertension. Hypertension 1999; 33: 1175–1178 10. Schunkert H, Hense HW, Doring A, Riegger GA, Siffert W. Association between a polymorphism in the G protein b3 subunit gene and lower renin and elevated diastolic blood pressure levels. Hypertension 1998; 32: 510–513 11. Beige J, Engeli S, Ringel J et al. Donor G protein b3 subunit 825TT genotype is associated with reduced kidney allograft survival. J Am Soc Nephrol 1999; 10: 1717–1721 12. Virchow S, Ansorge N, Rubben H, Siffert G, Siffert W. Enhanced fMLP-stimulated chemotaxis in human neutrophils from individuals carrying the G protein b3 subunit 825 T-allele. FEBS Lett 1998; 436: 155–158 13. Virchow S, Ansorge N, Rosskopf D, Rubben H, Siffert W. The G protein b3 subunit splice variant Gb3-s causes enhanced chemotaxis of human neutrophils in response to interleukin-8. Naunyn Schmiedebergs Arch Pharmacol 1999; 360: 27–32 14. Fogarty DG, Zychma MJ, Scott LJ, Warram JH, Krolewski AS. The C825T polymorphism in the human G-protein b3 subunit gene is not associated with diabetic nephropathy in type I diabetes mellitus. Diabetologia 1998; 41: 1304–1308 15. Bluthner M, Schmidt S, Siffert W et al. Increased frequency of G-protein b3-subunit 825 T allele in dialyzed patients with type 2 diabetes. Kidney Int 1999; 55: 1247–1250 Received for publication: 20.9.99 Accepted in revised form: 22.5.00.
(5)
Figure

Documents relatifs