Use of coronary angiography and revascularization
procedures following acute myocardial infarction
A European perspective
K. L Woods*, D. Ketley*, A. Agusti†, C. Hagn‡, R. Kala§, N. B. Karatzas
|
,
A. Leizorowicz¶, A. Reikvam**, J. Schilling††, R. Seabra-Gomes‡‡,
D. Vasiliauskas§§ and L. Wilhelmsen
\\
*Division of Clinical Pharmacology, Leicester Royal Infirmary, Leicester, U.K.; †Department of Clinical Pharmacology, CSU Vall Hebron, Barcelona, Spain; ‡Clinic for Internal Medicine, University of Innsbruck,
Innsbruck, Austria; §Maria Hospital, Helsinki, Finland;0Hygeia Hospital, Athens, Greece; ¶Unite de Pharmacologie Clinique, Lyon, France; **Research Forum, Ulleval University Hospital, Oslo, Norway; ††Institute
for Social and Preventive Medicine, University of Zurich, Zurich, Switzerland; ‡‡Intituto do Corac¸a˜o, Linda-A-Velha, Portugal; §§Laboratory for Cardiovascular Rehabilitation, Kaunas, Lithuania;00Department of
Medicine, O} stra Hospital, Go¨teborg, Sweden
AimsThere is little evidence to inform routine practice in
the use of coronary angiography and revascularization procedures after acute myocardial infarction. Large di ffer-ences in the uptake of these procedures have been reported but representative data are scarce. Outcome studies have produced opposing conclusions concerning the impact of the high rate of these cardiac procedures.
Methods and Results A population-based patient
sampling approach was utilized to identify routine practice in representative samples from 11 European countries. Data were collected retrospectively on treatment in the 6 months following acute myocardial infarction (n=2807). There was wide variation in utilization of coronary angi-ography and revascularization procedures. Even after restricting the analysis to patients <65 years (n=1262), there remained a 6–13 fold variation in the use of these procedures. A decreased likelihood of undergoing these
procedures was associated with older age. In addition, there was an independent and negative association between female sex and utilization of coronary angiography and coronary artery bypass grafting (CABG).
ConclusionThe effect on patient outcome of the observed
variation in use of these procedures is not known but has important cost and resource implications for the health services. Outcome research is needed to define patient selection criteria and to measure the cost-utility of different angiography and revascularization rates.
(Eur Heart J 1998; 19: 1348–1354)
Key Words: Myocardial infarction, revascularization,
coronary angiography.
See page 1274 for the Editorial comment on this article
Introduction
There is little evidence to guide the appropriate use of coronary angiography and revascularization procedures following acute myocardial infarction. This situation contrasts with the wealth of evidence which has been
gathered on pharmacological secondary prevention. In practice, coronary angiography is performed on a selected group of patients but there is little agreement as to the appropriate selection criteria[1,2].
Not surprisingly, large differences in the up-take of these procedures have been reported but rep-resentative data are scarce. The utilization of these non-pharmacotherapy strategies has not been studied in the typical, non-selected population of patients admitted to hospital with acute myocardial infarc-tion. In addition, the small number of outcome studies published have produced opposing conclusions
Revision submitted 15 February 1998, and accepted 25 February 1998.
Correspondence: Professor K. L. Woods, Department of Medicine
and Therapeutics, Robert Kilpatrick Clinical Sciences Building, Leicester Royal Infirmary, Leicester LE2 7LX, U.K.
enrolled in the European Secondary Prevention Study.
Method
Study sample
Eleven geographically defined European regions (median population 1·6 million, total source population 19·8 million) containing a mix of urban and rural settings, and of teaching and non-teaching hospitals provided representative study samples. All acute myo-cardial infarction patients (or in one region a 50% random sample of all) discharged from, or who died in, hospital with the main discharge diagnosis of acute myocardial infarction during a defined interval of January 1993–June 1994 were studied. The samples represented typical practice within the region from which they were taken and have been described pre-viously[7,8]. Cohorts of patients were followed from
hospital admission to follow-up 6 months later (2807 patients total) to identify typical practice.
Data retrieval
In all but one region the patient was contacted directly, 6 months after the index infarction, usually by telephone or alternatively by letter or at a clinic visit. Information from the patient was supplemented if necessary by data from physicians obtained by telephone or letter. Because of privacy laws in Switzerland, patients could not be approached directly; data were collected by letter to the treating physician. A standard data collection form, translated as necessary, was used. Before entry into the study database, anonymised forms were checked for completeness.
Statistical analysis
The observed use of cardiac invasive procedures is reported as a proportion. Associations between use of the strategies and patient age were estimated by the odds ratio (OR) and its 95% confidence interval (95% CI). Stratified analysis using Mantel–Haenszel OR in 5-year strata (<60, 60–64, 65–69, 70–74, 75–79, d80) was performed to examine the influence of sex on treatment while controlling for confounding by age. The reference group is stated for each analysis. Associations between
Results
Of the 4035 patients recruited, 3453 patients were discharged alive, and of these 271 patients died in the 6 months following acute myocardial infarction and another 375 patients were lost to the study. Six month follow-up data were therefore available for 2807 patients, 88% of known or possible survivors at 6 months. Loss to follow-up in different regions ranged from 2–31% (median 7%) of the original sample dis-charged alive[8]. For patients available for follow-up at
6 months post acute myocardial infarction, the data were 99·5% complete for coronary angiography and the revascularization procedures.
Utilization of coronary angiography and
revascularization procedures
The proportion of patients having coronary angio-graphy within 6 months of acute myocardial infarction varied between samples from 8% to 61% (Fig. 1). For coronary angioplasty (PTCA) the proportions were 1–28% (Fig. 2) and for coronary artery bypass grafting (CABG) the proportions were 1–20% (Fig. 3). Even after restricting the analysis to patients <65 years (n=1262), there remained a 6–13 fold variation in the use of coronary angiography (13–79%), PTCA (3–38%) and CABG (2–26%) (Figs 1–3).
Factors associated with the utilization of
coronary angiography and revascularization
procedures
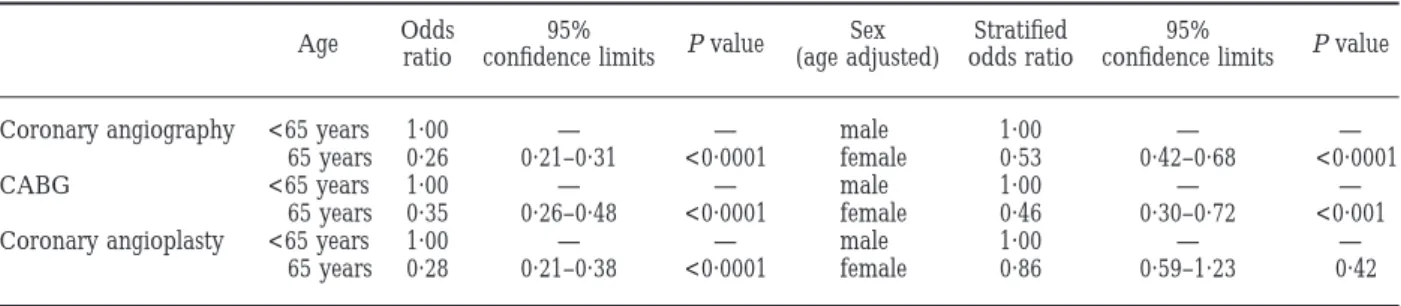
Utilization of all three procedures in all samples was greater in patients less than 65 years (Figs 1–3). The Spanish sample was an exception where the proportions having PTCA and CABG were constant, although very small, for both age groups. For the study sample as a whole, older age was associated with a significantly decreased likelihood of use of the three cardiac proce-dures (Table 1). In addition, there was an independent and negative association between female sex and utiliz-ation of coronary angiography and CABG. After con-trolling for the confounding effect of age, a highly significant and negative female sex effect remained for use of coronary angiography and CABG (Table 1). The association between coronary angioplasty and sex was not significant (Table 1). Amongst those patients who had a coronary angiogram in the 6 months following
acute myocardial infarction, there was no significant effect of sex on access to revascularization procedures after controlling for the confounding effect of age. As data on clinical indications for these procedures could not be collected, more detailed analysis was not possible. Exploration of the association between use of these strategies and use of pharmacotherapy approaches was performed to identify if countries with high use of pharmacological agents also demonstrated greater use of cardiac interventions in patients after acute myocardial infarction. Regression analysis and rank correlation revealed no significant relationship between either short-fall in thrombolytic use on admission or in beta blocker use at discharge and use of coronary angiography, PTCA or CABG in patients known to be alive at 6 months.
Discussion
This study has demonstrated and quantified a substan-tial disparity in the use of coronary angiography and revascularization procedures across 11 representative European samples in 1993–1994. The difference re-mained when the analysis was restricted to younger patients. This description of practice is at a point in time set against a changing situation for at least some of the
countries[9]. International variations in practice in the
use of cardiac interventions have been reported from Europe for all indications[10] and between Canada and
the U.S.A. following acute myocardial infarction, where a more interventionist pattern of care is observed[3,6]. A
recent study comparing use of cardiac procedures in two population based cohorts of elderly patients, hospital-ized after acute myocardial infarction, reported that rates of use of the procedures varied 5·2–7·8 fold between the U.S.A. and Canada[6]. In addition to
international differences, significant variation within countries in the uptake of cardiac procedures has been reported from both the U.K.[11,12]and the U.S.A.[4].
As might be expected, older age was associated with decreased use of angiography and revascularization procedures. Age was identified as the variable most predictive of use of angiography when statistical models were used to study patients who received thrombolysis in the GUSTO-1 study[13]. In the present study, in
addition to older age, female sex was found to be a significant factor associated with decreased access to invasive cardiac procedures; a negative influence of female sex on use of coronary angiography and CABG but not on PTCA was identified. It was not possible to control for other possible confounding clinical covariates. There are conflicting published reports on the effect of sex on use of these cardiac procedures.
100 0 Percentage use 80 60 40 20 United Kingdom Finland Spain Norway Sweden Lithuania Switzerland Greece
Portugal France Austria
Figure 1 Utilization of coronary angiography in the 6 months after acute myocardial infarction in all
Under-referral of women for coronary angiography has been well documented[14–16] but interestingly does not
appear to lead to lower subsequent use of revasculariza-tion procedures[14,16,17]. Supporting evidence comes
from a register of 33 359 patients that showed no gender difference in use of revascularization following coronary angiography[2]. Conversely, a difference in the treatment
of men and women was clearly identified in an American study in which observed rates of use of coronary angio-graphy and revascularization were adjusted to allow for important covariates. The study documented that men were more likely to undergo invasive cardiac procedures, including coronary angiography, than women[18]. It is
not known whether these differences represent appropri-ate levels of care for men and women or under-use in women or over-use in men. A recent review of this issue concluded that on current evidence it was premature to state that women were ‘discriminated’ against, as once coronary angiography was performed women were treated equitably[19]. However, the apparent disparity
in the treatment of men and women as illustrated in our data, particularly regarding in use of coronary angiography, warrants further study.
Why did such variation in use of these cardiac procedures occur? A major influencing factor in the utilization of coronary angiography and revasculariz-ation is availability of specialist facilities[13,20,21] and
staff[22]. Availability of resources may encourage use or
over-use of these procedures. Alternatively, belief in the need for facilities will drive their availability. Differences in waiting lists for these procedures might also influence the results reported in this study, as data were collected at one time point (6 months) after acute myocardial infarction. Disagreement on the benefits of these pro-cedures among physicians in different countries may contribute to the variation in their use. Philosophical differences were identified as the reason for variation in coronary angiography referral patterns in the U.K.[1] and possibly also for the variation in use of
revascularization following coronary angiography[2].
Coronary anatomy was identified as the most important predictor of the use and type of revascularization when statistical modelling was applied to patients recruited to the GUSTO-1 study[13].
Interestingly, there appeared to be no association between use of coronary angiography, PTCA or CABG with shortfall in prescribing pharmacotherapy strategies. This indicates that the approach to pharmacotherapy and non-pharmacotherapy strategies differed and suggests an absence of a consistently high or low ‘inter-ventionist’ culture. This observation is supported by study of a large health maintenance organisation where increased rates of angiography were associated with increased use of revascularization procedures, but not
0 Percentage use 30 20 10 United Kingdom Finland Spain Norway Sweden Lithuania Switzerland Greece
Portugal France Austria
Figure 2 Utilization of coronary angioplasty in the 6 months after acute myocardial infarction in all
with thrombolytic use or with recommended discharge medication[5].
There is a lack of strong evidence that higher rates of intervention result in improved patient outcome. A population based study of use of cardiac procedures and outcomes in elderly patients post acute myocardial infarction did not find better long-term survival rates for U.S.A. patients, with a more than five-fold higher rate of use of cardiac procedures, than Canadian patients with lower intervention rates. Although 30 day mor-tality rates were slightly, but significantly, lower for the U.S.A., the 1 year mortality rates were almost identical[6]. Similarly greater use of revascularization
procedures during index hospitalization for acute myo-cardial infarction, in Minnesota compared to southern Germany did not translate into survival difference at 28 days or 1 year following acute myocardial infarction[23].
In a comparison of cardiac procedure use after acute myocardial infarction in Texas and New York states, it was concluded that on average, there was no advantage with respect to mortality or health-related quality of life to performing the procedures at the higher rate identified in Texas[4].
However, although higher rates of intervention may not be clearly associated with lower mortality rates they may lead to better functional status[24]. A study of
50 0 Percentage use 40 30 20 10 United Kingdom Finland Spain Norway Sweden Lithuania Switzerland Greece
Portugal Austria France
Figure 3 Utilization of coronary artery bypass grafting in the 6 months after acute myocardial infarction
in all patients and patients less than 65 years in 11 European samples. =all patients; = <65 years.
Table 1 Association of use of coronary angiography and revascularization procedures with age, and with sex after adjustment for age (Mantel Haenzsel odds ratio in 5 year strata)
Age Oddsratio confidence limits95% P value (age adjusted)Sex odds ratioStratified confidence limits95% P value
Coronary angiography <65 years 1·00 — — male 1·00 — —
d65 years 0·26 0·21–0·31 <0·0001 female 0·53 0·42–0·68 <0·0001 CABG <65 years 1·00 — — male 1·00 — —
d65 years 0·35 0·26–0·48 <0·0001 female 0·46 0·30–0·72 <0·001 Coronary angioplasty <65 years 1·00 — — male 1·00 — —
d65 years 0·28 0·21–0·38 <0·0001 female 0·86 0·59–1·23 0·42 CABG, Coronary artery bypass grafting.
While it is possible that over-use may occur, it is also conceivable that procedures may be under-used in some groups of patients who would be likely to benefit, as was recently demonstrated when the RAND necessity criteria for angiography were applied to patients in a large Health Maintenance Organization[5]. Data from
the U.S.A. suggest that following thrombolytic therapy, patients at low cardiac risk are selected for intervention rather than the higher risk patients who would be most likely to benefit[13]. Identification of groups of patients
most likely to benefit from procedures would allow targeting of resources to that group.
Health economic modelling has indicated that there are patient subgroups in whom routine coronary angiography after acute myocardial infarction and treat-ment guided by its results is cost effective when com-pared to other strategies[25]. Further research is needed
to estimate the effectiveness and cost-effectiveness of alternative post acute myocardial infarction interven-tional strategies in different healthcare settings[26]. The
wide variations in European practice documented in the present study emphasize the need for outcome data to inform practice.
The European Secondary Prevention Study was funded within the BIOMED 1 programme of the European Union.
References
[1] Gray D, Hampton JR. Variations in the use of coronary angiography in three cities in the Trent Region. Br Heart J 1994; 71: 474–8.
[2] Henderson RA, Raskino CL, Hampton JR. Variations in the use of coronary arteriography in the UK: the RITA trial coronary arteriogram register. Q J Med 1995; 88: 167–73.
[3] Mark DB, Naylor CD, Hlaky MA et al. Use of medical resources and quality of life after acute myocardial infarction in Canada and the United States. N Engl J Med 1994; 331: 1130–5.
[4] Guadagnoli E, Hauptman PJ, Ayanian JZ, Pashos CL, McNeil BJ, Cleary PD. Variation in the use of cardiac procedures after myocardial infarction. N Engl J Med 1995; 333: 573–8.
[5] Selby JV, Fireman BH, Lundstrom RJ et al. Variation among hospitals in coronary angiography practices and outcomes after myocardial infarction in a large health maintenance organization. N Engl J Med 1996; 335: 1888–96.
[6] Tu JV, Pashos CL, Naylor CD et al. Use of cardiac pro-cedures and outcomes in elderly patients with myocardial infarction in the United States and Canada. N Engl J Med 1997; 336: 1500–5.
[7] The European Secondary Prevention Study Group. Translation of clinical trials into practice: a European
[11] Black N, Langham S, Petticrew M. Coronary artery bypass grafting and coronary angioplasty. Access to and availability of specialist services. Report of a CSAG working group. HMSO, London 1993.
[12] Black N, Langham S, Coshall C, Parker J. Impact of the 1991 NHS reforms on the availability and use of coronary revascularisation in the UK (1987–1995). Heart 1996; 76: 1–30.
[13] Pilote L, Miller DP, Califf RM, Rao JS, Weaver WD, Topol EJ. Determinants of the use of coronary angiography and revascularization after thrombolysis for acute myocardial infarction. N Engl J Med 1996; 335: 1198–205.
[14] Steingart RM, Packer M, Hamm P et al. Sex differences in the management of coronary artery disease. N Engl J Med 1991; 325: 226–30.
[15] Kee F. Referrals for coronary angiography in a high risk population. Quality in Health Care 1993; 2: 87–90.
[16] Gottleib S, Mazouz B, Keren A, Khoury Z, Stern S. Is there a gender bias in the pre-discharge and early post-myocardial infarction assessment? Eur Heart J 1995; 16 (Abstract Suppl): 225.
[17] Kee F, Gaffney B. Priority for coronary artery surgery: who gets by-passed when demand outstrips capacity? Q J Med 1995; 88: 15–22.
[18] Ayanian JZ, Epstein AM. Differences in the use of procedures between women and men hospitalized for coronary heart disease. N Engl J Med 1991; 325: 221–5.
[19] Kee F. Gender bias in treatment for coronary heart disease: fact or fallacy? Q J Med 1995; 88: 587–96.
[20] Every NR, Larson EB, Litwin PE for the Myocardial Infarc-tion Triage and IntervenInfarc-tion Project Investigators. The association between on-site cardiac catheterization facilities and the use of coronary angiography after acute myocardial infarction. N Engl J Med 1993; 329: 546–51.
[21] Behar S, Hod H, Benari B, Narinsky R, Pauzner H, Rechavia E, for the Israeli Thrombolytic Survey group. On-site cath-eterization laboratory and prognosis after acute myocardial infarction. Arch Int Med 1995; 155: 813–7.
[22] Jollis JG, DeLong ER, Peterson ED et al. Outcome of acute myocardial infarction according to the specialty of the admitting physician. N Engl J Med 1996; 335: 1880–7. [23] Shahar E, Lewis M, Keil U, McGovern PG, Lowel H,
Luepker RV. Hospital care and survival of acute myocardial infarction patients in Minnesota and southern Germany: a comparative study. Coronary Artery Dis 1996; 7: 467–73. [24] Pilote L, Racine N, Hlatky MA. Differences in the treatment
of myocardial infarction in the United States and Canada. Arch Int Med 1994 154; 1090–6.
[25] Kuntz KM, Tsevat J, Goldman L, Weinstein MC. Cost-effectiveness of routine coronary angiography after acute myocardial infarction. Circulation 1996; 94: 957–65. [26] Krumholz HM. Cardiac procedures, outcomes and
accountability. N Engl J Med 1997; 336: 1522–3.
Appendix
We thank the following for their participation in the study:
Austria — M. Angerer, F. Dienstl, R. Eiter, J. Mayr. Finland — E. Hussi, S Ja¨gerholm, A. Kohvakka, C-J. Lindstro¨m, K. Luomanma¨ki, V. Naukkarinen, S. Nurmilaukas-Rosenberg, O. Suhonen, P. Viikinkoski. France — C. Combe, G. Dayoub, C. Guerin, M. Lopez, P. Touboul, B. Veyre.
Greece — P. Antonatos, M. Avramides, S. Christakos, A. Deliyannis, I. Dernelis, S. Georgiades, I. Goudevenos, A. Hadjizacharias, K. Karides, K. Kifnides, C. Klrpizidas, G. Kollios, A. Kontopoulos, M. Koutmerides, T. Makris, B. Mikikes, G. Papazachariou, D. Simeonides, D. Sideris, A. Stavrides, L. Stergiou, T. Tsaknakis, A. Tyrologos, P. Vogiatzi.
Lithuania — V. Grizas, A. Jakubauskas, R. Kadziuiene, R. Raugaliene.
Norway — O. Anfinsen, E. Anker, E. Arnesen, N. Borge, H. Dørum, K. Fossum, D. Krohn Hansen, V. Høeg, K. Landmark, A. Myklebust, O. Ørjavik.
Portugal — A. Antunes, V. Arau´jo, J. Calqueiro, M. Carrageta, J. Correia, L. Correia, V. D’almeida, J. Fernandes, J. Ferreira, N. Gonc¸alves, V. Martins, M. Mendes, L. Parreira, L. Santos.
Spain — J. Arnau, G. Calvo, E. Cucurull, M. Farre, J. Llinares, S. Mateu, L. Molina, R. Morros, P. Roset. Sweden — M. Falkman.
Switzerland — P. Buehler, F. Follath, A. Frei, C. Gurtner, F. Gutzwiller, C. Hess, M. Knoblauch, R. Malacrida, P. Moehr, O. Oelz, M. Schwendinger, M. Staeubli.
United Kingdom — S. Fletcher, S. Wright.
And all the patients and staff who contributed to the data collection.