Archives of Disease inChildhood, 1981, 56, 775-778
Changing blood culture
isolates in
a
referral
neonatal
intensive
care
unit
O BATTISTI, RUTH MITCHISON, AND PAMELA A DAVIES
Department ofPaediatricsandNeonatal Medicine,HammersmithHospital, andDepartmentof Bacteriologyand Histopathology,Royal Postgraduate MedicalSchool,London
SUMMARY An
analysis
wasmade
of all cases ofbacteraemia
that had occurred in the referralneonatal intensivecare unitat
Hammersmith Hospital
during
theyears1976-79.
One hundred andthirteen
infants had positive blood cultures;
27 were born in thehospital,
and 86 admitted fromelsewhere.
Thisgave arate of5.7/1000
livehospital births,
and 165/1000outborn admissions totheunit.
The latter infants
werepredominantly
ofverylowbirthweight
or wereill.Thirty-three
oftheisolates
werecultured
in thefirst 48 hours of life(early)
and theremaining
80afterthat time(later).
Staphylococcus epidermidis
wastheorganism
mostoften isolated bothearly
and later. These resultswere
different
fromthose
recorded in theprevious
9 years(1967-75)
from the same unit.Then,
groupB3-haemolytic
streptococcuswasthe organism
mostoften isolatedearly,
whileGram-negative
bacteria
predominated
amonglaterisolates.
Thechanging
nature ofcare maycontribute to thesefindings.
Bacteraemia continues to bean important cause of
morbidity andmortality in neonatal intensive care
units, andperiodic review ofcasesmayhelptostress anychanging trends in theinfecting organisms, and in the newborn host. It also serves to monitor to someextentthesafety of various forms of care. In a previous survey from Hammersmith Hospital for the years 1967-75
inclusive,1
the group BP-haemolytic streptococcus was found to be the
organismmostoften isolatedinthefirst 48 hoursof
life. After that time however, Gram-negative isolateswere morethantwice ascommonas Gram-positive ones (H Jeffery et al., 1977, unpublished
data). We have now analysed results from the
succeeding 4 years, and report a changing pattern ofinfection.
Patientsandmethods
The infants studied were (1) the 4737live births of mothers deliveredinthe
maternity
unit of Hammer-smith Hospital between the years 1976 and 1979inclusive, and(2) the 521 newborn infants admitted from other hospitals and elsewhere to the referral neonatal intensivecareunit duringthesameperiod.
The latter infants were almost entirely of low
birthweightsor wereill;most wereboth.Duringthe study period 598 of the4737inborn infantswerealso
admitted to the intensive care unit.Theproportion of lowbirthweight infants born in the hospital is much higher than for the country as a whole, for many mothers in premature labourarereferredfrom other hospitals, and the socioeconomic status of the population served by the hospital is generally low. Blood was drawn for culture from a peripheral vein whenever possible as part of the routine investigations for suspected infection before anti-microbial therapy was started. Infection was suspected ifinfants were ill at birth and had come from an infected intrauterine environment; if they
werefebrile,orpresentedwithsigns such as lethargy, poorfeeding, vomiting, diarrhoea, unusual jaundice, and recurrent apnoea; or if there were suspicious
findings on clinical examination. Blood was also drawn forculture, usually by direct cardiac puncture, immediately after death in infants dying, whether or notthedeath was suspected of being infective. The
skin at the site ofvenous or cardiac puncture was prepared by careful swabbing with 70% isopropyl alcohol. The blood specimens were inoculated into
asetof twoorthree bottles, onecontaining tryptone soya broth andincluding an agar slope (Castaneda), and the other one or two containingthioglycollate broth.
The records of all infants with positive blood cultures were reviewed, and details of their clinical 775
776 Battisti,Mitchison, andDavies
course abstracted. The isolates were divided into
those occurring in the first 48 hours of life (early infection) andthose occurring after that time(later infection).Comparisonsweremade with the previous
study (H Jefferyetal., 1977,unpublished data),1 in
which the indications for blood culture had been
identical.
An antibiotic spray containing polymyxin,
bacitracin, and neomycin was applied to the
infant's umbilical cord at birth (or on admission
fromelsewhere) and once daily thereafter until the
cord separated. No antibacterial substance was
appliedtothe skin untiltheinfant waswell enough
to be bathed or had been transferred from an
incubatortoacot.Chlorhexidinewasthen used, but
inevery casethiswas sometimeafter blood hadbeen drawn for culture. Thisroutine forcord andskinhas been unchanged for many years except that
chlor-hexidine was substituted for hexachlorophane in
1971,the fifthyearof theprevious 9-yearsurvey.'
Results
One hundredand thirteen of the 5258 infantscared
forhadpositiveblood cultures:in27inborn infants (giving a rate of5 7/1000 for live hospital births)
andin 86 outborninfants (givingarateof165/1000
for outborn admissions to the neonatal unit).
These figures must be taken as a minimum rather
than as an exactestimate for we cannot be certain that our routine for taking blood cultures was
followed inevery case. Some infantsadmitted from elsewhere, for instance, were already receiving
antimicrobialtherapyonenteringthe unit.
Clinical details. Details of the 113 infantsaregiven
inTable 1. Themeantime ofisolation in theearly
and latercases was 34 6hours, and24-4 2 7
days respectively. Many of the later infections occurred beyondthe strict confines of the neonatal
period (first28days)andwere amonginfantsofvery
low birthweights and immature gestations who stayedinthenurseryformanyweeks after birth.
Table1 Clinical detailsofJJ3infants
Earlyinfection Laterinfection
(n=33) (n=80) Boys 19 50 Girls 14 30 Birthweight (kg) Mean(±SD) 1.52(10.65) 1.46(10-47) Range 0.77-33 57 0.62-2.3 Gestation(weeks) Mean(1SD) 31-3(±6 5) 30-9(±103) Range 26-40 26-40
Infecting organisms. Details of the nature of the
isolates are given in Table 2. It can be seen that
Staphylococcus epidermidis predominated in early and later infections.Itwasisolated from34(38
%)
of90infants who had drips inserted intoperipheral or
central veins, or had umbilical artery catheters passed.Itwashoweverrecoveredonlyfrom outborn
infants in the first 48 hours of life. Early group B
P-haemolytic
streptococcus and Staphylococcusaureus isolates were similarly confined to outborn infants.
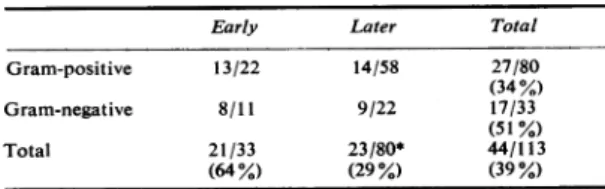
Mortality. Death was more common among early infected infants, and among those from whom
Gram-negativerather thanGram-positive organisms
wereisolated, whether earlyorlater(Table 3.)
Comparison with 1967-75 analysis. Expressing resultsas isolatesper yearfor thetwo unequaltime
periods 1967-75 (H Jeffery et al., 1977, unpub-lished data)1 and 1976-79 (Table 4) the
pre-valenceofGram-negative organismshasnotchanged appreciably-6-0compared with8 2 isolatesayear
respectively. This istrue both for early (2-6 v 2 7)
and later isolates(3 *4v5* 5).Gram-positive isolates
howeverhave increased from3-2 ayearin 1967-75
to20ayearin 1976-79(P<0.01).The increase isnot
significantamong earlyisolates(2-6v5 5),but it is
Table 2 Natureof isolates
Isolates Nunmberof isolates
Early Later
Gram-positive(n=80)
Staphylococcusepidermidis 8 47
Staphylococcusaureus 1 4
Group B,-haemolyticstreptococcus 6 1
Other* 7 6 Gram-negative(n=33) Escherichiacoli 1 5 Pseudomonasaeruginosa 3 5 Klebsiella-Enterobacter-Serratia group 0 5 Othert 7 7
*Micrococci,diphtheroids,non-haemolyticstreptococci. tAerobicsporebearers,Acinetobactersp,Bacteroidessp.
Table3 Mortality.(Numbers of deathsandisolates)
Early Later Total
Gram-positive 13/22 14/58 27/80 (34%) Gram-negative 8/11 9/22 17/33 (51%) Total 21/33 23/80* 44/113 (64%) (29%) (39%)
*Deathoccurredsignificantlymoreoften amongallearly infections thanamongall laterinfections(P<0.05).
Changing bloodcultureisolatesinareferralneonatalintensivecareunit 777
Table 4 Comparison ofisolates 1967-75and
1976-79.
(Figures expressed asisolates/year)Isolates 1967-75 1976-79 Gram-positive 3.2 20-0* Early 2.6 5-5 Later 0.6 14-5* Gram-negative 6.0 8.2 Early 2*6 2.7 Later 3.4 5. 5
*Differencessignificant (P<0-01-with Yates's correction for small
numbers).
Table5
Results
for1967-75compared with thosefor 1976-791967-75 1976-79
Rate/1000livehospital
births 1*6 5-7 Rate/1000 outside admissions(illor infantsoflow birthweight) 76 165 Medianbirthweight (kg) 1-6 1.3 Predominantisolate
Early GroupB,3-haemolytic Staphylococcuis
streptococcus epidermidis
Later Escherichia coli Staphylococcus epidermidis
so among later isolates (0-6 v 14-5) (P<0-01). A
summaryof the main differences between theperiods
1967-75 and 1976-79 isgivenin Table 5.
Discussion
Achangein thepatternof bacterial isolates cultured
from the blood stream of infants nursed in the
referralneonatal intensivecareunitatHammersmith
Hospital has taken place during the last fewyears.
Gram-positive organisms are nowforemost among
both early and later infections, whereas in the
preceding 9 years Gram-negative isolates were
equally prevalent among early infections and
completelydominatedthe later infections. Astriking
recent increase in isolation of S. epidermidis is
largely responsiblefor thischange.
Thisorganism,askincommensal,isrecognisedas an important coloniser ofcerebrospinal fluid shunt systems and indwelling catheters.2 Its ability to
produce virulence factors andtodevelop antibiotic resistance isnow morewidely appreciated,3anditis
becoming acknowledgedas a causeofmajorinfection
among otherwise normalchildren.4 It hasgenerally
been dismissedas acontaminant when isolated from newborn blood cultures in the past,56although its occasional significance for preterm infants, albeit
withalowmorbidityandmortality, hasbeennoted
bysome.7 Weareinnodoubt about itspathogenicity
for many ofourinfants. Ten of the 55 babies with positive cultures forS. epidermidis also had clinical and radiological evidence ofpneumonia, but other associated illness-such as meningitis or urinary tract infections-was not seen. The picture more commonly presented was that ofavery immature
infant having total parenteral nutrition suddenly becoming less well with recurrent apnoea and
significant neutropenia. The majority of these recovered with prompt use ofantimicrobial therapy and the removal of centrally placed intravenous catheters. Others with positive cultures for this organism who appeared only mildly ill frequently hadapronouncedneutrophilleucocytosis.
In astudy ofcolonisationpatternsfrom a neonatal intensive care unit, it, together with S. aureus and
Gram-negative enteric
bacilli,
was considered an abnormalpharyngeal inhabitant.8 A high colonisa-tion rate by methicillin-resistant S. epidermidis has also beenassociated withanoutbreakof bacteraemia in anothernewborn intensivecareunit where the use of antibiotics was widespread, according to a preliminaryreport.9
A survey from Yale10 where careful records of neonatal bacteraemia have been kept for 50 years, also suggestsa recentincrease of S. epidermidis isolates, togetherwith other unusual bacteria. It has been recovered from the bloodstreamof12%of infants'failingtothrive' and from
12% of jaundiced infants in a maternity nursery wherenormal infants had sterilecultures;11attempts
at identification of the isolates suggested there was moresimilaritybetweenthose frombloodstream and
nasopharynx,than betweenbloodstreamandskin.12
Possiblereasonsfor the
finding
inoursurveyhaveto besought in thetreatment ofthe newborn host, andin the host himself. During 1976-79,there were
more very low
birthweight
infants (<1500 g)admitted tothe unit fromelsewhere,mostofwhom
were ill. An unusual number of very immature
infantswasalso born in the
hospital,
and the medianbirthweight
of the 113 infants studiedwas1F3
kg.The inability of the most immature to mount a
satisfactory
immune-inflammatory
response is wellknown.13
Inaddition
toumbilical arterycatheterisa-tionfor blood gasmonitoringwhich has beenthought
necessary for many of them, there has been a
steadilyincreasinguse of total parenteral nutrition,
and ofintravenous dripsingeneral.
Ninety
percentofthestudy infantshad hadacatheterpassedinto
an umbilical or central blood vessel or had an
infusion needle into aperipheral vein,andeither of thesewasretained there for
varying periods.
Further detailedanalysisof the associationbetweeninfection,
778 Battisti,Mitchison,and Davies
drug therapy, umbilical vessel catherisation, and intravenous infusions is being conducted pro-spectively. Although every effort is made toconduct the insertion of drip needles and catheters in a
sterilefield, the inevitable technical difficulties witha
few of the tiniest babies maymitigate against this. Howeverit is clear that themostmeticulouspractical
technique, together with stringent and frequent reviewof all aspects of drip and catheter care are nowheremorenecessarythan inaneonatalintensive care unit if the chance of infections due to S.
epidermidis and other skin contaminants is to be lessened. Random checks of the infusion fluids used have not suggested contamination. Others have reported itas acommonenvironmentalcontaminant of milkdripfeeds.'4
Overuseof antimicrobialtherapy in neonatal units isrecognised15 and is to someextentinevitable. At
presentabout 52%ofinfantsinourreferral nursery
aretreated with suchdrugs,and in the first 6months of 1980 several strains of S.epidermidis resistant to all thecommonlyused antibiotics have beenfound. Careof the umbilicuspractised by us-theuse ofa
polymyxin,bacitracin,andneomycin spray-has been
unchangedin thehospitalfor well over 15 years. This too could possibly be furthering the hold of the
organism in the unit. The skin has been found to
become
profusely
colonised by coagulase-negative staphylococci when powders containingchlor-hexidine or hexachlorophane are used to control
colonisationbyS.aureus.'6
One final aspect of this survey which is more
encouraging, although possibly fortuitous,is the fact that amonginborn infantsduring 1976-79, there has beenno case ofearly group B
3-haemolytic
strep-tococcus bacteraemia. This organism was the most frequent cause ofearlybacteraemiaduring 1967-75, and had a high mortality. It still occurs among outborn infants. Since 1975 at HammersmithHospital, when surgical induction of labour proves necessary, it is first ascertained whenever possible whether or not the mother is a carrier for
3-haemolyticstreptococcus. Ifthis proves to be the
casetheinduction andsubsequentlabour are covered with
penicillin.
In addition to these measures, ourobstetriciansarenowcarrying out surgical induction less frequently. Treatment of selected mothers17
seems to be a more hopeful solution to this
devastatingfetal and neonatalillness than treatment of theinfants,often started too late to be effective.
References
Jeffery H, MitchisonR, WigglesworthJ S,Davies P A. Early neonatal bacteraemia. Comparison of group B streptococcal, other Gram-positive and Gram-negative infections.Arch DisChild1977; 52:683-6.
2 Feigin R D, Shearer W T. Opportunistic infection in
children. I. Inthecompromised host. J Pediatr 1975; 87: 507-14.
3 Marsik F J, Parisi J T. Significance ofStaphylococcus
epidermidis in the clinical laboratory. Appl Microbiol 1973; 25: 11-4.
4 Feigin R D, Shearer W T. Opportunistic infection in children. III. In the normal host. J Pediatr 1975; 87: 852-66.
5 DunhamEC.Septicemiain thenewborn.Am JDisChild 1933; 45: 229-53.
6 Eitzman D V, Smith R T. Thesignificance of bloodcultures in thenewbornperiod-Am JDisChild1957;94: 601-3. Buetow K C, Klein S W, Lane R B. Septicemia in premature infants. The characteristics, treatment, and
prevention of septicemiain premature infants. Am J Dis Child 1965; 110: 29-41.
8 SpruntK,Leidy G, RedmanW.Abnormal colonization ofneonatesinanintensivecareunit: means ofidentifying
neonates at risk of infection. Pediatr Res 1978; 12: 998-1002.
9 BernickJ J,Baublis J V, Borer R C. Nosocomial bac-teremiain neonates(abstract). PediatrRes1979; 13: 388. 10 Freedman R M, Ingram D L, Gross I, Ehrenkranz R A, Warshaw J B,BaltimoreR S. Ahalf century ofneonatal
sepsisatYork 1928 to 1978. Am J Dis Child1981; 140: 140-4.
1 ClymoAB,HurleyR, Norman A P.Coagulase-negative
staphylococci from the blood ofneonates (abstract). J
Clin Pathol1971;24:477.
12 Clymo A B. Distribution ofcoagulase-negative
staphy-lococci fromnewborns (abstract).JClinPathol 1971; 24: 770.
13 Miller M E. Hostdefensesinthe humanneonate.
Mono-graphs in Neonatology. NewYork: Grune & Stratton,
1978:1-9.
14 SchreinerRL, Eitzen H, GfellMA,etal.Environmental contamination of continuous drip feedings. Pediatrics
1979;63: 232-7.
15 HammerschlagMR, KleinJ0,Herschel M, Chen F C J,
FerminR. Patternsofuseofantibioticsin twonewborn nurseries.NEnglJMed 1977; 296: 1268-9.
16 Alder V G, Burman D, Simpson R A, Fysh J,
Gillespie W A. Comparison of hexachlorophane and
chlorhexidinepowdersinprevention of neonatalinfection.
ArchDisChild1980;55:277-80.
17 Yow M D, Mason E 0, Leeds L J, Thompson P K,
ClarkDJ,Gardner S E.Ampicillinpreventsintrapartum transmission ofgroup BStreptococcus. JAMA 1979;241: 1245-7.
Correspondenceto DrPamelaADavies, Department ofPaediatrics and Neonatal Medicine, Hammersmith
Hospital,DuCane Road, London W12 OHS.