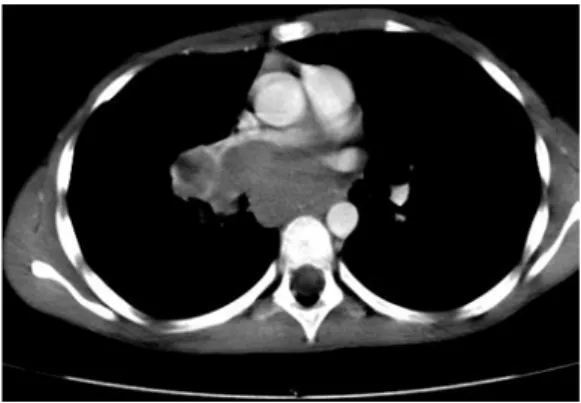
Burkitt's lymphoma with bilateral cavernous sinus and mediastinal involvement in a child
3
0
0
Texte intégral
Figure
Documents relatifs