Colonic tuberculosis in an immunocompetent patient
The MIT Faculty has made this article openly available.
Please share
how this access benefits you. Your story matters.
Citation
Zubieta-O’Farrill, Gregorio, Juan de Dios del Castillo-Calcaneo,
Carlos Gonzalez-Sanchez, Eduardo Villanueva-Saenz, and Jacob A.
Donoghue. “Colonic Tuberculosis in an Immunocompetent Patient.”
International Journal of Surgery Case Reports 4, no. 4 (2013): 359–
361. © 2013 Surgical Associates Ltd.
As Published
http://dx.doi.org/10.1016/j.ijscr.2013.01.018
Publisher
Elsevier
Version
Final published version
Citable link
http://hdl.handle.net/1721.1/90415
Terms of Use
Article is available under a Creative Commons license; see
publisher’s site for details.
CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports4 (2013) 359–361
ContentslistsavailableatSciVerseScienceDirect
International
Journal
of
Surgery
Case
Reports
jo u r n al h om ep a g e :w w w . e l s e v i e r . c o m / l o c a t e / i j s c r
Colonic
tuberculosis
in
an
immunocompetent
patient
Gregorio
Zubieta-O’Farrill
a,∗,
Juan
de
Dios
del
Castillo-Calcáneo
a,
Carlos
Gonzalez-Sanchez
b,
Eduardo
Villanueva-Saenz
a,c,
Jacob
A.
Donoghue
daSurgeryDepartment,AngelesPedregalHospital,MéxicoCity,Mexico bGastroenterologyDepartment,AngelesPedregalHospital,MéxicoCity,Mexico cColon&RectumDepartment,AngelesPedregalHospital,MéxicoCity,Mexico
dDivisionofHealthSciencesandTechnology,HarvardMedicalSchoolandMassachusettsInstituteofTechnology,Boston,UnitedStates
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received9December2012
Receivedinrevisedform10January2013 Accepted22January2013
Available online 4 February 2013 Keywords:
Colonictuberculosis Tuberculosis
Colonoscopyintuberculosis
Tuberculosisinimmunocompetentsubjects
a
b
s
t
r
a
c
t
INTRODUCTION:One-thirdoftheworld’spopulationisinfectedwithtuberculosis(TB),withintestinal TBrepresentingthesixthmostcommonpresentationofextrapulmonaryTB.Thediagnosisofintestinal TBisachallengeforphysiciansduetoitsdiverseclinicalmanifestationsthatmimicotherinfectious, autoimmune,andneoplasticdisorders,andisthusrarelyconsideredasthecausativeagentofdisease. PRESENTATIONOFCASE:Wepresenta55-year-oldmalewithnorelevantfamilialhistory,whopresented duetoalossof10kgofweightin2monthsaccompaniedbynocturnaldiaphoresisandcontinuous abdominaldistension.
DISCUSSION:TheincidenceandtheseverityofintestinalTBareincreasedinimmunosuppressedpatients andmorerapidlyprogressduetodeficientimmuneresponse.However,ourimmunocompetenthad severeprogressionresultinginsurgerylessthanamonthafterthediagnosiswasmade.
CONCLUSION:WhilethediagnosisofintestinalTB,andspecificallycolonicTB,isdifficultandisalmost neverthefirstdiagnosisentertainedoutsidetheimmunocompromisedpopulation,wepresentarare caseinwhichthediseasepresentsinanimmunocompetentpatient.
© 2013 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
1. Introduction
One-thirdoftheworld’spopulationisinfectedwith tubercu-losis(TB),withintestinalTBrepresentingthesixthmostcommon presentationofextrapulmonaryTB.1ThediagnosisofintestinalTB
isa challengefor physiciansduetoitsdiverseclinical manifes-tationsthatmimicotherinfectious,autoimmune,andneoplastic disorders,andisthusrarelyconsideredasthecausativeagentof disease.Therefore,ahighindexofsuspicionisessentialtoreach thecorrectdiagnosis.
2. Casereport
Wepresenta55-year-oldmalewithnorelevantfamilial his-tory,whopresentedduetoalossof10kgofweightin2months accompaniedbynocturnaldiaphoresisandcontinuousabdominal distension.
Hewasadmittedtoourhospitalforstudies.Hiscompleteblood count(CBC)showedmicrocyticanemiaandafecaloccultblood testwasperformedandreturnedpositive.Thesefindingsprompted colonoscopy and gastroesophagoduodenoscopy, which revealed
∗ Correspondingauthorat:AngelesPedregalHospital,CaminoaSantaTeresa 1055,Col.HeroesdePadierna,MagdalenaContreras,MexicoCity,DF,Mexico. Tel.:+5215539556584.
E-mailaddress:[email protected](G.Zubieta-O’Farrill).
chronicgastritisandacoloniculcerthatextendedthroughoutthe rightcolon(Fig.1).
Biopsies were taken from the ulcerated area of the colon. Histopathologicalanalysisdemonstratedanacuteinfectious pro-cess and a chronic infectious process with the presence of granulomas(Figs.2and3).Thepathologicreportsuggestedthe diagnosticpossibilityoftuberculosisandpolymerasechain reac-tionofthesamesampleconfirmedthepresenceofMycobacterium tuberculosisDNA.
HIV testing was confirmed negative. A positive PPD test provoked an indurationof 12mm in the forearmat 12h post-inoculationandachestX-raywasreportedasnormal.Thesubject was discharged with Rifater (rifampin/isoniazid/pyrazinamide) understrictsupervision.
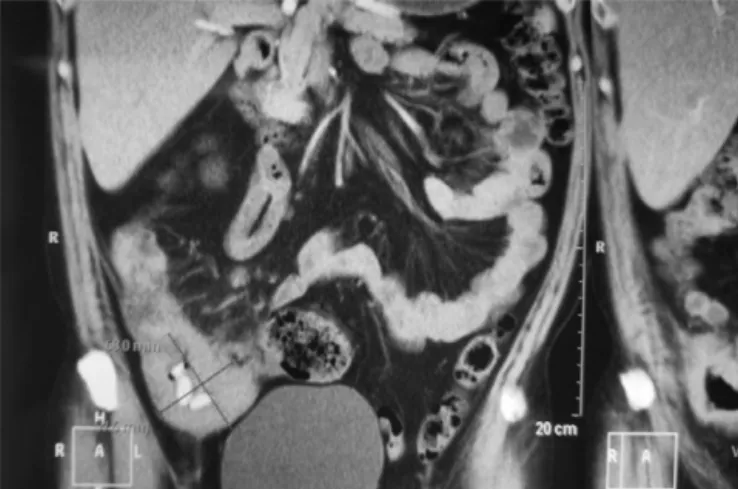
Twomonthsafterthepatientwasdischarged,hepresentedto theemergencydepartmentwithabdominalpainintheleftlower quadrant,accompaniedbytachycardia,bloodystools,reboundand tenderness,andanabdominalCTwasperformed.Imaging discov-eredanabdominalmassobstructingtherightcolonattheileocecal valve(Fig.4)andsurgicalinterventionwasimmediatelyprepared. Arighthemicolectomywithileotransversal anastomosiswas performed,withpathologicevaluationoftherightcolon demon-strating the colonic mass to be filled with granulomas and characteristicmultinucleatedgiantcells.Thepatienthada satis-factoryevolutionandwasdischarged.
At1yearfollow-upthepatientisdoingwellandhasfinished hiscourseofRifatertreatment.
2210-2612/$–seefrontmatter © 2013 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
CASE
REPORT
–
OPEN
ACCESS
360 G.Zubieta-O’Farrilletal./InternationalJournalofSurgeryCaseReports4 (2013) 359–361
Fig.1.Colonoscopyimageshowinganulcerthatextendsthroughouttherightcolon.
Fig.2. Granulomaincolonbiopsywithmultinucleatedgiantcells.
Fig.3. Granulomaincolonatthecenterofalymphoidfollicle.
Fig.4.AbdominalCTshowinganobstructivemassintherightcolon,attheileocecal valve.
3. Discussion
TheincidenceandtheseverityofintestinalTBareincreased inimmunosuppressedpatientsandmorerapidlyprogressdueto deficient immuneresponses.1 However,ourimmunocompetent
patienthadsevereprogressionthatresultedinsurgerylessthan amonthafterthediagnosiswasmade.
Incaseseriesreportedpreviously,themainsymptomsreported inpatientswithintestinalTBarechronicabdominalpain,fever, weight loss,changes in bowel habits, abdominal mass, ascites, nausea,and vomiting.2 In ourpatient,only twoof thesemajor
symptomswerepresent,withweightlossbeingthemainreason forconsultation.
Conventional laboratory tests are nonspecific and do not contribute to the differential diagnosis. Elevated erythrocyte sedimentation rate,highC-reactive protein levels, anemia, and lymphopeniaorlymphocytosisarecommonlaboratoryfindings.3
Inourpatient,CBC showedanemia andorientedthephysicians towardapossiblegastrointestinalbleeding.Positivefecaloccult bloodtestpromptedthecolonoscopyweperformed,whichledus totheultimatediagnosis.
Ulcersarethemostcommoncolonoscopyfindinginpatients withdiagnosedcolonicTB,presentinginasmanyas70%ofthese patients.4Ourpatientdemonstratedthesesamecharacteristicsin
hiscolonoscopy.
Granulomasare found in biopsies in up to54% of all cases reportedbyAlvaresetal.,4andarethemostcommon
histopatho-logicallesionincolonicTB.Theselesionswerealsoreportedforour patient.Eventhoughgranulomasoccurinbothintuberculosisand Crohn’sdisease,caseationcharacteristicallytypifiestuberculosis. Caseationmaybeseeninthelymphnodeswithoutconcomitant caseation in the colonic biopsy; additionally, it may be totally absentinthosewhohavereceivedantituberculartherapyinthe past.5Inourcase,caseationwasnotreportedbythepathologist.
PCRisoneoftheconfirmatorydiagnostictestsusedwhenthereis diagnosticdoubtbetweenTBandotherdiseases.4Histopathologic
analysissuggestedcolonicTBasadiagnosticprobability,leading ustoorderthePCRtestofthesamespecimen.Thepositive pres-enceofMycobacteriumtuberculosisDNAconclusivelyconfirmedour diagnosisofcolonicTB.
TheMantoux test is positive in 70–86%of patients, but has limitedusefulnessinimmunosuppressedpatients.5Inourcase,the
Mantouxtestreturnedpositive,whichisexpectedinan immuno-competentindividual.
AminorityofpatientswithintestinalTBreportpriorhistoryof TBinfectionyetmorethan50%haveanormalchestX-ray.4 Our
CASE
REPORT
–
OPEN
ACCESS
G.Zubieta-O’Farrilletal./InternationalJournalofSurgeryCaseReports4 (2013) 359–361 361
patienthadanormalchestX-rayandnoprevioushistoryofTB, which,asreported,isnotuncommon.
4. Conclusion
WhilethediagnosisofintestinalTB,andspecificallycolonicTB, isdifficultandisalmostneverthefirstdiagnosisentertained out-sidetheimmunocompromisedpopulation,wepresentararecase inwhich thediseasepresentsinanimmunocompetentpatient. However,asratesoftuberculosisriseandasmanyasone-thirdof theworld’spopulationarealreadyinfected,intestinalTBshouldbe consideredonthedifferentialdiagnosisofpatientspresentingwith similarsequelaeofintestinaldisease.Ourcaseillustratesthat,while uncommon,intestinalTBcanhaveatorpidcourseevenrequiring emergencysurgerydespiteadequatetreatment.
Disclosure
Thepatientconsentwasobtainedatthefirsthospitalization;our localethicscommitteereviewedthecasepriortoitssubmissionfor publication.
Conflictofintereststatement
Noconflictofinterestforanyoftheauthorsinthiscasereport.
Funding
Nofundingwasreceivedspecificallyforthisstudy.
JacobDonoghueissupportedbyawardNumberT32GM007753 fromtheNationalInstituteofGeneralMedicalSciences.Thecontent
issolelytheresponsibilityoftheauthorsanddoesnot necessar-ilyrepresenttheofficialviewsoftheNationalInstituteofGeneral MedicalSciencesortheNationalInstitutesofHealth.
Ethicalapproval
Writteninformedconsentwasobtainedfromthepatientfor publicationofthiscasereportandaccompanyingimages.Acopy ofthewrittenconsentisavailableforreviewbytheEditor-in-Chief ofthisjournalonrequest.
Authorcontributions
GregorioZubieta-O’Farrillperformeddatacollectionand anal-ysis.Juan de Dios delCastillo-Calcáneo diddatacollection and writing.CarlosGonzalez-Sanchezand EduardoVillanueva-Saenz did data collection while Jacob A. Donoghue did the writing job.
References
1.DonoghueHD,HoltonJ.Intestinaltuberculosis.CurrentOpinioninInvestigational Drugs2009;22:490–6.
2.RasheedS,ZinicolaR,WatsonD,BajwaA,McDonaldPJ.Intra-abdominaland gastrointestinaltuberculosis.ColorectalDisease2007;9:773–83.
3.Muneef MA, Memish Z, Mahmoud SA, Sadoon SA, Bannatyne R, Khan Y. Tuberculosisinthebelly:areviewofforty-sixcasesinvolvingthe gastroin-testinaltractandperitoneum.ScandinavianJournalofGastroenterology2001;36: 528–32.
4.AlvaresJF,DevarbhaviH,MakhijaP,RaoS,KottoorR.Clinical,colonoscopic, andhistologicalprofileofcolonictuberculosisinatertiaryhospital.Endoscopy 2005;37:351–6.
5. HorvathKD,WhelanRL.Intestinaltuberculosis:returnofanolddisease.American JournalofGastroenterology1998;93:692–6.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.