Validity and reliability on three European
language versions of the Safety
Organizing Scale
DIETMAR AUSSERHOFER1, MARIA SCHUBERT2, MARY BLEGEN3, SABINA DE GEEST1
AND RENÉ SCHWENDIMANN1
1
Institute of Nursing Science, University of Basel, Basel, Switzerland,2Centre of Clinical Nursing Science, University Hospital Zurich,
Switzerland, and3School of Nursing–UCSF, San Francisco, 94143 CA, USA
Address reprint requests to: René Schwendimann, Institute of Nursing Science, University of Basel, Bernoullistrasse 28, CH-4056 Basel, Switzerland. Tel: +41-61-267-09-19; Fax: +41-61-267-09-55; E-mail: rene.schwendimann@unibas.ch
Accepted for publication 2 December 2012
Abstract
Background. The Safety Organizing Scale (SOS) offers a reliable snapshot of nurses’ engagement in unit-level safety behaviors in hospitals. As no comparable questionnaire exists in German, French and Italian, we explored the psychometric properties of SOS translations into each of those languages.
Design and Methods. The psychometric properties of the nine-item SOS were tested according to American Educational Research Association guidelines.
Subjects and Setting. Between October 2009 and June 2010, 1633 registered medical and/or surgical nurses in 35 Swiss hospitals completed translated SOS questionnaires.
Results. For each translation, psychometric evaluation revealed evidence based on content (scale-content validity index >0.89), response patterns (e.g. average of missing values across all items = 0.80%), internal structure (e.g. comparative fit indices >0.90, root mean square error of approximation <0.08) and reliability (Cronbach’s alpha >0.79). We differentiated the scale regarding one related concept (implicit rationing of nursing care). Higher SOS scores correlated with supportive leader-ship and lower nurse-reported medication errors, but not with nurse-reported patient falls.
Conclusions. The SOS offers a valuable measurement of engagement in safety practices that might influence patient outcomes. Initial evidence regarding the validity and reliability of the translated versions supports their use in German, French and Italian. Concurrent validity will require confirmation via further analysis using more reliable outcome measures (e.g. mortality rates). The translated versions’ predictive validity needs to be established in prospective studies.
Keywords: high reliability, safety organizing, patient safety behaviors, psychometric evaluation, Swiss hospitals
Introduction
In the past years, it has become obvious that quality and patient safety are major challenges for health care [1–3]. According to patient safety experts, developing a‘safety culture’ is a founda-tion for overcoming current safety and quality problems in health care [4–6]. Numerous conceptual definitions exist for safety culture, most of which originated in high-risk industries [7,8]. For instance, safety culture within health-care organiza-tions can be defined as a ‘subset of organizational culture which relates specifically to the values and beliefs concerning patient safety’ [9]. As values and beliefs can vary significantly across departments and across units within the same health-care or-ganization [10, 11], a ‘lived safety culture’ must be visible as reflected by observable safety behaviors within each unit [12].
Safety culture and high reliability
Despite many improvements, health care is still struggling in creating a culture that sustains high levels of safety and quality performance over time [13]. Research on‘high-reliability organi-zations’ revealed that a key feature of their safety culture that facilitates the maintenance of excellent performances is ‘collect-ive mindfulness’ [14]. To stay mindful, despite hazardous envir-onments, frontline employees consider constantlyfive principles: tracking small failures, resisting oversimplification, remaining sensitive to operations, maintaining capabilities for resilience and taking advantage of shifting locations of expertise [13, 14]. Studying ‘collective mindfulness’ in health care could help to better understand health-care professionals’ behaviors under-lying a patient safety culture [12] and might be a fruitful pathway leading to maintenance of safety performance over time [13].
Measuring the reliability of health-care organizations
The Safety Organizing Scale (SOS) [12], developed by Vogus and Sutcliffe, corresponds to such interrelated behavioral safety processes of ‘collective mindfulness’ [12]. The SOS is a 1D instrument backed by high-reliability organizational theory. The nine items assess the extent to which registered nurses (RNs) and their colleagues engage in safety behaviors and practices on their unit. Previous evidence supports the SOS’s strong psychometric properties [12].
As no validated safety culture questionnaire existed in German, French and Italian, the SOS’s psychometric excel-lence and 1D structure made it a strong candidate for cross-cultural testing. In addition, replication of studies under new conditions increases external generalizability of findings and the validity of the underlying theory [15]; if results on the SOS could be confirmed in a different cultural context, the underlying theory of high-reliability organizations in health care and the measurement of it by the SOS would be sup-ported. To measure safety culture across a national sample of Swiss hospitals, we translated the SOS into German, French and Italian and then used the translated versions within the framework of the Swiss RN4CAST study (Nurse Forecasting: Human Resources Planning in Nursing). We surveyed RNs, as they represent the largest subgroup of health-care profes-sionals in hospitals and play a major role in guaranteeing patient safety [16–18].
This study aims to explore the psychometric properties of the German, Italian and French versions of the SOS by translating the instrument and assessing its reliability and validity in new settings.
Methods
DesignThis is a sub-study of the Swiss RN4CAST study, a multicentre cross-sectional study within the EU Seventh Framework (EU Project number: 223468).
Setting and sample
RNs working on medical, surgical and mixed medical– surgical wards of Swiss acute-care hospitals were surveyed. Hospitals were sampled according to a quota sample method based on language region and hospital type (university, can-tonal and regional hospitals with ≥60 beds and ≥50 RNs). For university and cantonal hospitals, random samples of 2–6 eligible wards were selected; for smaller regional hospi-tals, all eligible wards were included to survey at least 50 RNs per hospital. All RNs active on the selected units were invited to participate.
Cross-cultural translation of the SOS
To adapt the SOS in a culturally relevant and comprehensible form while maintaining its original meaning and intent [19],
we translated the SOS according to the adapted Brislin model [20]—an iterative process involving forward–backward translation and expert group discussion. The seven-point Likert response scale was retained. Following back transla-tion, our expert group identified no inconsistencies in any item’s meaning or wording.
Validity and reliability testing
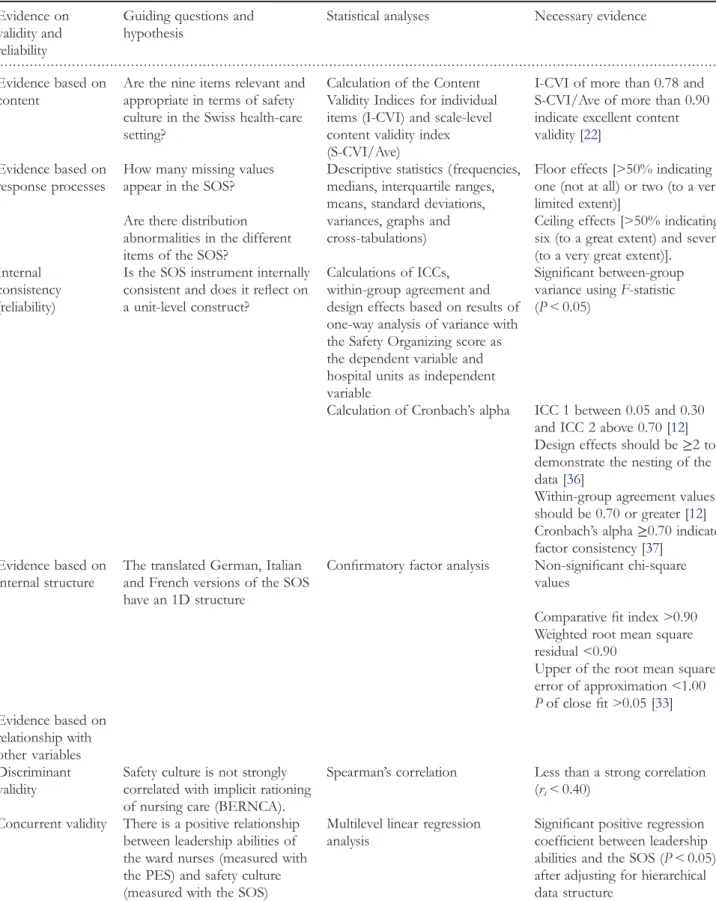
Our general objective was to determine whether German, French and Italian versions of the SOS would reveal psycho-metric properties similar to those of the original. Therefore, our validation strategy was based on that of Vogus and Sutcliffe [12]. Following American Educational Research Association guidelines, [21] we developed questions and hypotheses that guided the testing of the three translations’ validity and reliability (see Table1).
Validity testing.After translating, we asked experienced RNs whether the SOS reflected a relevant content domain. For each language version, 10 experienced RNs were asked to rate the extent to which the SOS reflected nurses’ safety behaviors. We established ‘evidence based on content’ by calculating the consensus estimates of the ratings of item scale relevance (content validity index of individual items and overall scale) [22].
‘Evidence based on response processes’ was compiled through assessment of distribution and skewing of the data, missing responses, multiple crosses for each item and overall scale and acceptability (number of respondents omitting no items).
To test the‘internal consistency’ of the measurements and the precision of test results, we calculated Cronbach’s alpha. Furthermore, to test whether the translated versions of the SOS reliably reflect a unit level construct—making aggrega-tion of data appropriate—we computed five measures. Using F-statistic from a one-way variance analysis, we calculated between-group variance. We applied two types of intraclass correlations (ICCs), to calculate the proportion of variance explainable by unit membership (ICC 1) and the reliability of unit means (ICC 2). Both measures describe how strongly responses from RNs in the same unit resemble each other. [12]. We also calculated design effects to account for within-group sample size, which could have inflated ICCs. The degree to which responses of individuals within a group are interchangeable was calculated with the within-group agreement [12].
To provide ‘evidence based on internal structure’, we aimed to confirm the 1D structure of the original (English) SOS [12]. To test whether our model would fit the data, we conducted confirmatory factor analysis.
We assessed ‘discriminant and concurrent validity’ to provide evidence of the relationships of the SOS with other variables. Both higher RNs’ engagement in safety behaviors and lower levels of implicit rationing of nursing care might be visible features of a safety culture and, therefore, related to each other. A recent study confirmed this assumption, suggesting that the extent to which individual RNs are ration-ing nursration-ing care might also depend on the prevailration-ing safety
. . . .
Table 1 Research questions and hypotheses of this validation study Evidence on
validity and reliability
Guiding questions and hypothesis
Statistical analyses Necessary evidence
Evidence based on content
Are the nine items relevant and appropriate in terms of safety culture in the Swiss health-care setting?
Calculation of the Content Validity Indices for individual items (I-CVI) and scale-level content validity index (S-CVI/Ave)
I-CVI of more than 0.78 and S-CVI/Ave of more than 0.90 indicate excellent content validity [22]
Evidence based on response processes
How many missing values appear in the SOS?
Descriptive statistics (frequencies, medians, interquartile ranges, means, standard deviations, variances, graphs and cross-tabulations)
Floor effects [>50% indicating one (not at all) or two (to a very limited extent)]
Are there distribution abnormalities in the different items of the SOS?
Ceiling effects [>50% indicating six (to a great extent) and seven (to a very great extent)]. Internal
consistency (reliability)
Is the SOS instrument internally consistent and does it reflect on a unit-level construct?
Calculations of ICCs, within-group agreement and design effects based on results of one-way analysis of variance with the Safety Organizing score as the dependent variable and hospital units as independent variable
Significant between-group variance using F-statistic (P < 0.05)
Calculation of Cronbach’s alpha ICC 1 between 0.05 and 0.30 and ICC 2 above 0.70 [12] Design effects should be≥2 to demonstrate the nesting of the data [36]
Within-group agreement values should be 0.70 or greater [12] Cronbach’s alpha ≥0.70 indicate factor consistency [37]
Evidence based on internal structure
The translated German, Italian and French versions of the SOS have an 1D structure
Confirmatory factor analysis Non-significant chi-square values
Comparativefit index >0.90 Weighted root mean square residual <0.90
Upper of the root mean square error of approximation <1.00 Pof closefit >0.05 [33] Evidence based on relationship with other variables Discriminant validity
Safety culture is not strongly correlated with implicit rationing of nursing care (BERNCA).
Spearman’s correlation Less than a strong correlation (rs< 0.40)
Concurrent validity There is a positive relationship between leadership abilities of the ward nurses (measured with the PES) and safety culture (measured with the SOS)
Multilevel linear regression analysis
Significant positive regression coefficient between leadership abilities and the SOS (P < 0.05) after adjusting for hierarchical data structure
culture, i.e. collective mindfulness [23]. Yet, implicit rationing of nursing care served as a comparison concept to explore whether the SOS is discriminant from this important factor determining patient safety and quality of care [24]. Vogus and Sutcliffe provided initial evidence that better leadership abilities of nurse managers and adequate staffing levels are associated with better safety culture and fewer adverse events such as medication errors and patient falls [12, 25]. To provide con-current validity for the translated versions of the SOS, we assessed these relationships in the Swiss cross-cultural setting.
Five variables were used for discriminant and concurrent validity testing:
Implicit rationing of nursing care, leadership abilities, staff-ing level, medication errors and patient falls.
Implicit rationing of nursing care, i.e. ‘the withholding of or failure to carry out necessary nursing measures for patients due to a lack of nursing resources (staffing, skill mix and time)’ was measured with the 32-item, 1D Basel Extent of Rationing of Nursing Care (BERNCA) instrument [24], which asks how often in their last 7 working days, nurses have been unable to carry out any of 32 listed necessary nursing tasks. Evidence is sup-porting the BERNCA’s validity and reliability [24]. Cronbach’s alphas for the German-, French- and Italian language versions were 0.94, confirming the internal consistency of this construct.
To assess leadership abilities, we used the ‘Nurse Manager Ability, Leadership, and Support’ subscale of the ‘Practice Environment Scale’ [26], which asks nurses whether specific leadership elements are present at their workplace. Psychometric strength of the practice envir-onment scale was reported in previous studies [26, 27]. Cronbach’s alphas for the German- and Italian versions were 0.76, for the French version, 0.80.
The staffing level and adverse outcomes were measured with RN self-report of the ‘nurse-to-patient ratio’ on
the last shift, and the frequency of ‘medication errors’ and‘patient falls’ on their units over the last year. These three variables matched single items from the instru-ment battery of the RN4CAST nurse questionnaire. All instruments and items (except the SOS) used in the Swiss RN4CAST study had been used in previous studies [28,29]. Data collection and data management
Data collection took place between 12 October 2009 and 30 June 2010. For each participating hospital, a pre-identified contact person (e.g. nursing expert, chief nursing officers) supported us in planning and conducting the data collection. Completed questionnaires were scanned, and data were sub-jected to quality control procedures.
Statistical analysis
The statistical analyses corresponding to our validity and reli-ability testing are listed in Table1. To evaluate the SOS’s in-ternal structure, we performed confirmatory factor analysis using MPlus (version 6.1, 2010, Muthen and Muthen).
Descriptive, correlation, reliability and variance analyses were performed using IBM SPSS Statistics (version 18.0.2; SPSS Inc., Chicago, IL, USA); regression analysis was per-formed with STATA (version 11/SE; StataCorp LP), whereas ICCs, design effects and within-group agreement were calculated with Microsoft Office Excel 2011®
. All hy-potheses were subjected to two-sided testing, whereby the level of significance was set at P < 0.05.
Ethical considerations
Surveyed RN consented to participate in the study by volun-tarily completing and returning the questionnaires. The study was approved by ethics committees representing all involved cantons. . . . . Table 1 Continued Evidence on validity and reliability
Guiding questions and hypothesis
Statistical analyses Necessary evidence
Concurrent validity There is a negative relationship between nurse-to-patient ratio and safety culture.
Multilevel linear regression analysis
Significant negative regression coefficient between leadership abilities and the SOS (P < 0.05) after adjusting for hierarchical data structure
Concurrent validity There is a negative relationship between safety climate and nurse-reported medication errors and patient falls
Multilevel logistic regression analysis
Significant odds for lower frequent nurse reports for medication errors and patient falls (odds ratios <1.00, P < 0.05) after adjusting for hierarchical data structure
Results
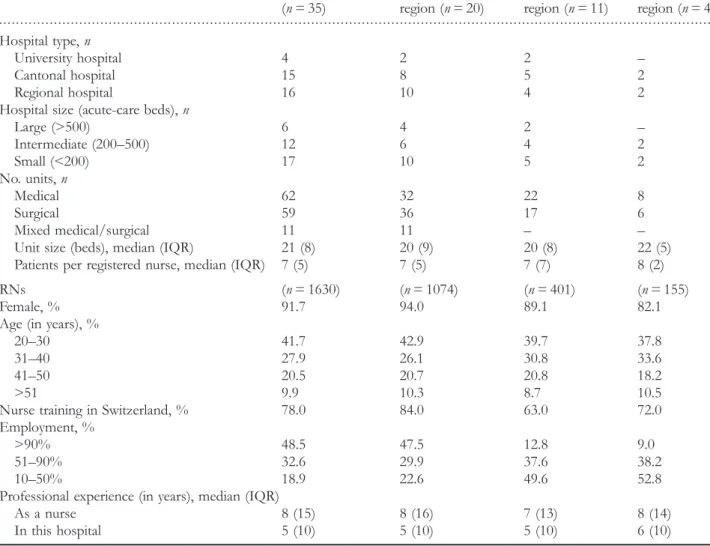
Questionnaires were completed and returned by 1633 RNs (overall response rate = 72%: German = 73%; French = 74%; Italian = 69%). Of these, 1630 (German = 1074; French = 401; Italian = 155) were eligible for statistical analyses (3 questionnaires were excluded from analysis as they could not be assigned to a unit). Characteristics of the participant sample are presented in Table2.
The content validity ratings for the three language versions of the SOS revealed the relevance of both the individual items and of the overall SOS scale. Content validity indices for individual items for the German version ranged from 0.6 (items 4) to 1.0 (items 2, 3 and 8); for the French version from 0.7 (item 7) to 1.0 (items 2, 6 and 8); and for the Italian version from 0.7 (items 3 and 7) to 1.0 (items 2, 6 and 8). Scale-level content validity index was 0.91 for the German and the French versions and 0.89 for the Italian version.
Frequencies of missing values were low, ranging from 0.4 to 1.9% (average = 0.8%). In all, 1564 RNs (95.8%) submit-ted questionnaires with no missing values. For confirmatory factor analysis, then, we used only data from complete questionnaires.
Mean item values on the seven-point scale ranged from 4.62 (standard deviation = 1.27; item 4) to 5.62 (standard deviation = 1.07; item 5). The mean for the entire scale (SOS score) was 5.11 (standard deviation = 0.91) and the median score was 5.22 (25–75th quartile = 4.56, 5.22 and 5.78). All nine items and the SOS score were slightly left skewed, and minor ceiling effects could be observed in items 5, 6 and 9.
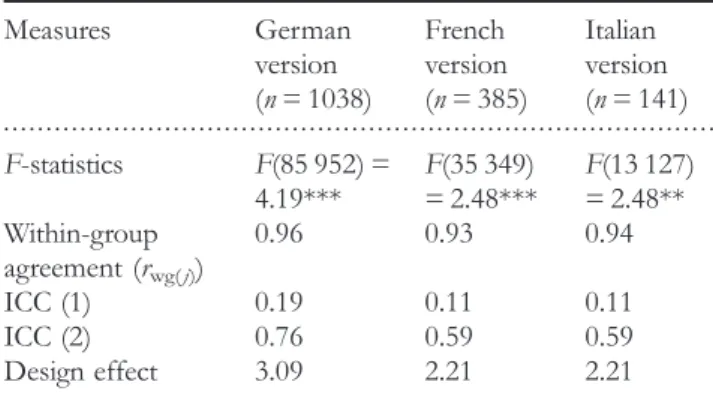
The alpha coefficients for this 1D construct were 0.90 (German), 0.92 (French) and 0.79 (Italian), indicating scale reliability. The reliability of the SOS as an aggregate unit measure was shown by the significant analysis of variance, within group agreement, ICC 1 and design effects (Table3). The ICC 2 scores were slightly below recommended levels for
. . . .
Table 2 Characteristics of the participating hospitals and RNs
Hospitals Total Switzerland
(n = 35) German-speaking region (n = 20) French-speaking region (n = 11) Italian-speaking region (n = 4) Hospital type, n University hospital 4 2 2 – Cantonal hospital 15 8 5 2 Regional hospital 16 10 4 2
Hospital size (acute-care beds), n
Large (>500) 6 4 2 – Intermediate (200–500) 12 6 4 2 Small (<200) 17 10 5 2 No. units, n Medical 62 32 22 8 Surgical 59 36 17 6 Mixed medical/surgical 11 11 – –
Unit size (beds), median (IQR) 21 (8) 20 (9) 20 (8) 22 (5)
Patients per registered nurse, median (IQR) 7 (5) 7 (5) 7 (7) 8 (2)
RNs (n = 1630) (n = 1074) (n = 401) (n = 155)
Female, % 91.7 94.0 89.1 82.1
Age (in years), %
20–30 41.7 42.9 39.7 37.8
31–40 27.9 26.1 30.8 33.6
41–50 20.5 20.7 20.8 18.2
>51 9.9 10.3 8.7 10.5
Nurse training in Switzerland, % 78.0 84.0 63.0 72.0
Employment, %
>90% 48.5 47.5 12.8 9.0
51–90% 32.6 29.9 37.6 38.2
10–50% 18.9 22.6 49.6 52.8
Professional experience (in years), median (IQR)
As a nurse 8 (15) 8 (16) 7 (13) 8 (14)
In this hospital 5 (10) 5 (10) 5 (10) 6 (10)
the French and Italian versions, which might be an effect of the lower average group size (RNs per unit) when compared with units of German-speaking hospitals. However, design effects and the other measures support the assumption that all translated SOS versions are meaningful at the unit level and justify the aggregation of individual responses to the unit level. For each language version, confirmatory factor analyses described the closest possible data fit. As Table 4 shows, items had highly significant factor loadings for all three ver-sions. For the German and French versions, our model demonstrated excellentfit across all fit indices; for the Italian version, we failed only to demonstrate an acceptable root mean square error of approximation (Table 4). In summary, these results provide evidence of the 1D structure of all three translated versions of the SOS and justify the aggrega-tion of the nine individual items to a single SOS score.
To show discriminant validity, correlation analysis between the SOS and the BERNCA revealed a weak, but statistically significant negative relationship for all three translations (German rs=−0.24 P < 0.01; French rs=−0.24, P < 0.01;
Italian rs=−0.28, P < 0.01). These results distinguish safety
culture, as measured with the SOS, from implicit rationing of nursing care.
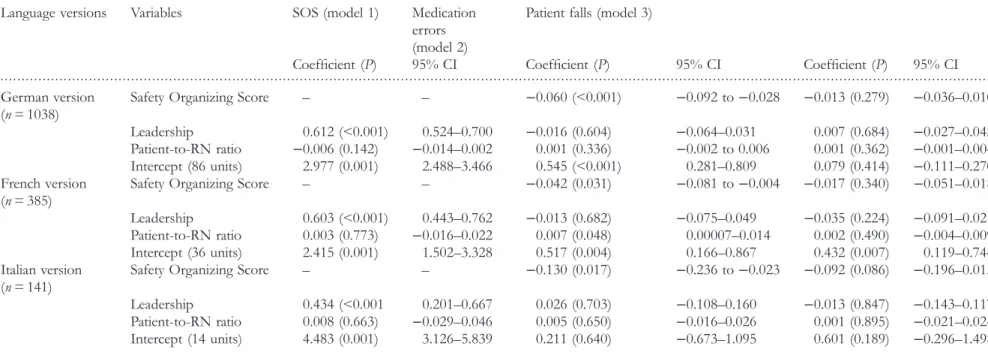
As reported in Table 5, concurrent validity was examined via several regression models. Thefirst shows the association of nurse-reported leadership and patient-to-RN ratios on the SOS Score. For all three translations, leadership was positive-ly related to the SOS, whereas no significant relationships were found between the patient-to-RN ratios and the SOS (Table 5). Model 2 shows that higher SOS scores were asso-ciated with lower nurse-reported medication errors for all three translations (German: odds ratio = 0.941; French: odds ratio = 0.959; Italian: odds ratio = 0.878), whereas in model 3, no SOS score was significantly related to patient falls in any language version (Table5).
Discussion
This study provides evidence supporting the validity and reli-ability of all three translated versions of the SOS, which we
tested in the cultural context of the Swiss health-care system, pursuing procedures conforming to rigorous international standards [21].
The SOS measures health-care professionals’ engagement in crucial safety behaviors at the unit level, reflecting the safety culture of health-care organizations. Most instruments measuring the patient safety culture are based on multidi-mensional conceptualizations [30,31] but capture few patient safety behaviors. In our understanding, safety culture is char-acterized by visible features of a safety culture [32], such as safety behaviors of professionals, that directly influence patient outcomes. The SOS’s quick diagnostic sampling of crucial patient safety behaviors reflecting on ‘collective mind-fulness’ makes it a valuable tool for monitoring the reliability of health-care organizations.
Overall, our results indicate similar psychometric properties to those for the original SOS. ‘Evidence based on content’ confirmed our accurate and rigorous translation process. This might have resulted in a low proportion of missing values and indicated the instrument’s practicability and acceptability (‘evi-dence based on response processes’). The observed slightly positive data skewing and ceiling effects for three out of nine items give little reason for concern (e.g. systematic measurement error), because all nine items still reflected variability across units. However, the SOS’s responsiveness to change needs to be explored in future safety and quality improvement research.
The structure of the tool as 1D was supported for all ver-sions. Item loadings on one factor were strong for all three versions. The one weak value was for the Italian SOS version; we failed to demonstrate adequate root mean square error of approximation. The root mean square error of ap-proximation depends on the sample size, represented in the denominator of its equation [33]. Although only a few para-meters required estimation, the sample size for the Italian version was likely not sufficient for an adequate estimation of this fit index and its confidence interval. Future studies should re-confirm the internal structure of the Italian version with a larger sample size.
Whereas we confirmed the hypothesis that supportive leadership was positively related with the SOS (H3), we found no association between the patient-to-RN ratio and the SOS (H4). The recall of the workload of each RN for the last shift might not be accurate, and there was little vari-ability in the data across the hospitals, making it difficult to show a relationship with the SOS. Similar to Vogus and Sutcliffe [12], SOS scores were inversely associated with nurse-reported medication errors, but, in contrast to their findings, we found no relationship with nurse-reported patient falls. We assume that the SOS might be less sensitive to this type of adverse events, as there are many patient-related risk factors triggering patient falls [34], which are dif-ficult to influence by RNs’ general safety behaviors. Our initial inconsistent findings on the relationship between the translated versions of the SOS and patient outcomes require confirmation via further analysis using more reliable outcome measures (e.g. mortality rates), as our nurse-reported patient outcomes may be subject to bias (recall bias) [35]. The RN4CAST study used a cross-sectional design, which does
. . . .
Table 3 Measures to determine the effect of data nesting of the SOS within hospital units
Measures German version (n = 1038) French version (n = 385) Italian version (n = 141) F-statistics F(85 952) = 4.19*** F(35 349) = 2.48*** F(13 127) = 2.48** Within-group agreement (rwg( j)) 0.96 0.93 0.94 ICC (1) 0.19 0.11 0.11 ICC (2) 0.76 0.59 0.59 Design effect 3.09 2.21 2.21 **P < 0.01, ***P < 0.001.
. . . .
Items of the SOS German
version (n = 1038) French version (n = 385) Italian version (n = 141)
Factor loadings Standard error Factor loadings Standard
error
Factor loadings
Standard error
We have a good‘map’ of each other’s talents and skills 0.708*** 0.018 0.760*** 0.026 0.402*** 0.068
We talk about mistakes and ways to learn from them 0.823*** 0.014 0.814*** 0.021 0.783*** 0.042
We discuss our unique skills with each other so we know who on the unit has relevant specialized skills and knowledge
0.828*** 0.012 0.859*** 0.016 0.762*** 0.044
We discuss alternatives as to how to go about our normal work activities
0.760*** 0.014 0.879*** 0.016 0.826*** 0.036
When giving report to an oncoming nurse, we usually discuss what to look out for
0.616*** 0.023 0.746*** 0.028 0.369*** 0.075
When attempting to resolve a problem, we take advantage of the unique skills of our colleagues
0.804*** 0.013 0.771*** 0.021 0.665*** 0.051
We spend time identifying activities we do not want to go wrong 0.630*** 0.021 0.653*** 0.029 0.742*** 0.038
When errors happen, we discuss how we could have prevented them 0.736*** 0.019 0.799*** 0.021 0.843*** 0.040
When a patient crisis occurs, we rapidly pool our collective expertise to attempt to resolve it
0.611*** 0.022 0.708*** 0.027 0.489*** 0.060
Chi-square 50.710*** 26.003* 24.811*
Degrees of freedom 13 13 13
Comparativefit index 0.997 0.998 0.993
Root mean square error of approximation (90% confidence interval) 0.053 (0.038,
0.069) 0.051 (0.021, 0.079) 0.080 (0.028, 0.128) Pof closefit 0.352 0.437 0.139
Weighted root mean square residual 0.462 0.319 0.375
*P < 0.05, ***P < 0.001. V alida tion sa fety organizing scale • Sa fety , methods, and interna tional compari sons 163
. . . .
Table 5 Multilevel regression analysis results for relationship of the SOS with other variables (concurrent validity)
Language versions Variables SOS (model 1) Medication
errors (model 2)
Patient falls (model 3)
Coefficient (P) 95% CI Coefficient (P) 95% CI Coefficient (P) 95% CI
German version (n = 1038)
Safety Organizing Score – – −0.060 (<0.001) −0.092 to −0.028 −0.013 (0.279) −0.036–0.010
Leadership 0.612 (<0.001) 0.524–0.700 −0.016 (0.604) −0.064–0.031 0.007 (0.684) −0.027–0.042
Patient-to-RN ratio −0.006 (0.142) −0.014–0.002 0.001 (0.336) −0.002 to 0.006 0.001 (0.362) −0.001–0.004
Intercept (86 units) 2.977 (0.001) 2.488–3.466 0.545 (<0.001) 0.281–0.809 0.079 (0.414) −0.111–0.270
French version (n = 385)
Safety Organizing Score – – −0.042 (0.031) −0.081 to −0.004 −0.017 (0.340) −0.051–0.018
Leadership 0.603 (<0.001) 0.443–0.762 −0.013 (0.682) −0.075–0.049 −0.035 (0.224) −0.091–0.021
Patient-to-RN ratio 0.003 (0.773) −0.016–0.022 0.007 (0.048) 0.00007–0.014 0.002 (0.490) −0.004–0.009
Intercept (36 units) 2.415 (0.001) 1.502–3.328 0.517 (0.004) 0.166–0.867 0.432 (0.007) 0.119–0.744
Italian version (n = 141)
Safety Organizing Score – – −0.130 (0.017) −0.236 to −0.023 −0.092 (0.086) −0.196–0.013
Leadership 0.434 (<0.001 0.201–0.667 0.026 (0.703) −0.108–0.160 −0.013 (0.847) −0.143–0.117
Patient-to-RN ratio 0.008 (0.663) −0.029–0.046 0.005 (0.650) −0.016–0.026 0.001 (0.895) −0.021–0.024
Intercept (14 units) 4.483 (0.001) 3.126–5.839 0.211 (0.640) −0.673–1.095 0.601 (0.189) −0.296–1.498
Multilevel linear (model 1) and logistic (models 2 and 3) regression analyses were performed with STATA 11 with unit-level random effects. Including the random effects accounts for the hierarchical structure of the data (RNs nested within units). Coefficient in model 1 refers to the unstandardized regression coefficients (B), in model 2 and 3 to logit coefficients. All models were adjusted for sociodemographic characteristics of RNs (age, education, employment grade and professional experience).
P, P-value; CI, confidence interval.
ofer
et
al
not allow deriving causal inferences between the SOS and patient outcomes. Predictive validity of the translated ver-sions of the SOS for patient safety outcomes needs to be established in future prospective studies.
Conclusions
In summary, the SOS is a valuable tool to measure RNs’ en-gagement in safety behaviors and processes with possible direct relationships to patient outcomes. Initial evidence on the validity and reliability of the translated SOS versions supports their use in German-, French- and Italian-speaking health-care settings. In clinical practice, it can be used to describe and monitor both the extent of health-care professionals’ engage-ment in the tested behaviors/processes and the prevailing ‘col-lective mindfulness’ at unit level. As the individual items entail information on changeable behaviors/processes, the SOS allows unit and hospital leaders to plan, implement and evalu-ate interventions to improve the safety culture [7].
With further validity testing of the German, French and Italian SOS versions, this measure can be used in outcome research to explain its interaction with other known outcome influencing factors such as rationing of nursing care or the nurse practice environment. This would augment our knowl-edge of the most significant factors of clinical practice related to patient safety and quality of care.
Acknowledgements
The authors thank all hospitals for participating in the Swiss RN4CAST study. Special thanks go to Tracy Glass, PhD (Biostatistician) for her statistical support and to Chris Shultis for his work of editing the article.
Funding
The research leading to these results has received funding from the European Union’s Seventh Framework Programme (FP7/2007–2013) under grant agreement no. 223468. For more information on the RN4CAST project, please visit www.rn4cast.eu.
References
1. Soop M, Fryksmark U, Koster M et al. The incidence of adverse events in Swedish hospitals: a retrospective medical
record review study. Int J Qual Health Care 2009;21:285–91.
2. Aranaz-Andres JM, Aibar-Remon C, Vitaller-Burillo J et al. Impact and preventability of adverse events in Spanish public hospitals: results of the Spanish National Study of Adverse
Events (ENEAS). Int J Qual Health Care 2009;21:408–14.
3. de Vries EN, Ramrattan MA, Smorenburg SM et al. The inci-dence and nature of in-hospital adverse events: a systematic
review. Qual Saf Health Care 2008;17:216–23.
4. Conen D. Maßnahmen zur Verbesserung der Patientensicherheit.
Bundesgesundheitsblatt–Gesundheitsforschung–Gesundheitsschutz 2011;54:
171–5.
5. Vincent C, Aylin P, Franklin BD et al. Is health care getting
safer? BMJ 2008;337:a2426.
6. Institute of Medicine. Patient Safety. Achieving a New Standard for Care. Washington, DC: The National Academies Press, 2004. 7. Halligan M, Zecevic A. Safety culture in healthcare: a review of
concepts, dimensions, measures and progress. BMJ Qual Saf
2011;20:338–43.
8. Guldenmund FW. The nature of safety culture: a review of
theory and research. Saf Sci 2000;34:215–57.
9. Feng X, Bobay K, Weiss M. Patient safety culture in nursing: a
dimensional concept analysis. J Adv Nurs 2008;63:310–9.
10. Deilkas E, Hofoss D. Patient safety culture lives in departments and wards: multilevel partitioning of variance in patient safety
culture. BMC Health Serv Res 2010;10:85.
11. Singer SJ, Gaba DM, Falwell A et al. Patient safety climate in 92 US hospitals: differences by work area and discipline. Med Care
2009;47:23–31.
12. Vogus TJ, Sutcliffe KM. The Safety Organizing Scale: develop-ment and validation of a behavioral measure of safety culture in
hospital nursing units. Med Care 2007;45:46–54.
13. Chassin MR, Loeb JM. The ongoing quality improvement journey:
next stop, high reliability. Health Aff (Millwood) 2011;30:559–68.
14. Weick KE, Sutcliffe KM. Managing the Unexpected: Resilient Performance in an Age of Uncertainty. 2nd edn. San Francisco, CA: John Wiley, 2009.
15. McKinley W. Organizational theory development: displacement
of ends? Organ Stud 2010;31:47–68.
16. Kendall-Gallagher D, Blegen MA. Competence and certification
of registered nurses and safety of patients in intensive care
units. Am J Crit Care 2009;18:106–13.
17. Teng CI, Dai YT, Shyu YI et al. Professional commitment, patient safety, and patient-perceived care quality. J Nurs Scholarsh
2009;41:301–9.
18. Aiken LH, Clarke SP, Cheung RB et al. Educational levels of
hospital nurses and surgical patient mortality. JAMA
2003;290:1617–23.
19. Sperber AD. Translation and validation of study instruments
for cross-cultural research. Gastroenterology 2004;126:S124–S8.
20. Jones PS, Lee JW, Phillips LR et al. An adaptation of Brislin’s
translation model for cross-cultural research. Nurs Res
2001;50:300–4.
21. American Educational Research Association. Standards for Educational and Psychological Testing. Washington DC: American Educational Research Association, 1999.
22. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indica-tor of content validity? Appraisal and recommendations. Res
Nurs Health2007;30:459–67.
23. Schubert M, Ausserhofer D, Desmedt M et al. Levels and cor-relates of implicit rationing of nursing care in Swiss acute care
24. Schubert M, Glass TR, Clarke SP et al. Validation of the basel extent of rationing of nursing care instrument. Nurs Res
2007;56:416–24.
25. Vogus TJ, Sutcliffe KM. The impact of safety organizing, trusted leadership, and care pathways on reported medication
errors in hospital nursing units. Med Care 2007;45:997–1002.
26. Lake ET. Development of the practice environment scale of the
Nursing Work Index. Res Nurs Health 2002;25:176–88.
27. Gajewski BJ, Boyle DK, Miller PA et al. A multilevel con
firma-tory factor analysis of the Practice Environment Scale: a case
study. Nurs Res 2010;59:147–53.
28. Schubert M, Glass TR, Clarke SP et al. Rationing of nursing care and its relationship to patient outcomes: the Swiss exten-sion of the International Hospital Outcomes Study. Int J Qual
Health Care2008;20:227–37.
29. Aiken LH, Clarke SP, Sloane DM. Hospital staffing,
organiza-tion, and quality of care: cross-national findings. Nurs Outlook
2002;50:187–94.
30. Sexton JB, Helmreich RL, Neilands TB et al. The Safety Attitudes Questionnaire: psychometric properties, benchmark-ing data, and emergbenchmark-ing research. BMC Health Serv Res
2006;6:44.
31. Nieva VF, Sorra J. Safety culture assessment: a tool for improv-ing patient safety in healthcare organizations. Qual Saf Health
Care2003;12:ii17–23.
32. Flin R, Mearns K, O’Connor P et al. Measuring safety
climate: identifying the common features. Saf Sci 2000;34:
177–92.
33. Kline RB. Principles and Practice of Structural Equation Modeling. 3rd edn. New York: The Guilford Press, 2011.
34. Cameron ID, Murray GR, Gillespie LD et al. Interventions
for preventing falls in older people in nursing care
facilities and hospitals. Cochrane Database Syst Rev 2010;20:
CD005465.
35. Singer S, Lin S, Falwell A et al. Relationship of safety climate
and safety performance in hospitals. Health Serv Res
2009;44:399–421.
36. Sorra JS, Dyer N. Multilevel psychometric properties of the AHRQ hospital survey on patient safety culture. BMC Health
Serv Res2010;10:199.
37. Pett M, Lackey N, Sullivan J. Making Sense of Factor Analysis:
The Use of Factor Analysis for Instrument Development in
Health Care Research. Thousand Oaks: Sage Publications, 2003.