Telemedicine for cardiac surgery candidates
4
0
0
Texte intégral
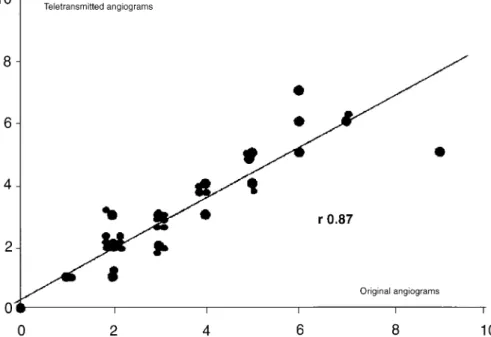
Figure
Documents relatifs