- PHONE CONTACT WITH
THE BLOOD BANK
-> MTP ACTIVATION
-> THAWING OF FFP
- PHONE CONTACT WITH
THE OR
- TRAUMA TEAM
(DOCTORS&NURSES)
CALLED IN THE
RESUSCITATION ROOM
INTRODUCTIONSevere trauma can cause life-threatening hemorrhage. This rare condition is worsened by the fact that actively bleeding trauma patients quickly develop trauma induced coagulopathy TIC. Thought to be the consequence of the “lethal triad” old concept (hypothermia, dilution, coagulopathy), this acute coagulopathy is in fact a more complex phenomenon and occurs at the early phase after trauma.
Bleeding trauma patients with TIC need extraordinary therapeutic measures consisting in emergent damage control surgery, damage control hemostatic resuscitation with massive transfusion, use of hemostatic agents, permissive hypotension and highly specific and qualified technical and human resources at patient’s arrival in the resuscitation room.
And to be efficient, all those strategies, often called Damage Control Resuscitation DCR, need to be applied as early as possible.
In order to identify bleeding and coagulopathic trauma patients before hospital admission, we have developed an easy-to-measure purely clinical score (the TICCS) aiming at “flagging” patients with TIC on the site of injury. In contrast to currently available trauma scoring systems, our score can be calculated by paramedics in less than 1 min and then communicated to the hospital allowing taking the necessary organisational measures before patient’s arrival. THE TICCS
The TICCS ranges from 0 to18. It is a 3-item based score considering (I) the severity of trauma (for 2 points), (II) its hemodynamic repercussions (for 5 points) and (III) the extent of the body injury (for 11 points).
- 2 points are attributed if the patient is judged critical. If he isn’t, no point is attributed.
- The patient gets 5 points if his pre-hospital systolic blood pressure is below 90 mmHg. 0 if SBP is always above 90 mmHg.
- 11 points are attributed for the extent of body injury, distributed like this: 1 point for head and neck, 1 point for each extremity, 2 points for the torso region, 2 points for abdominal region and 2 points for the pelvic region.
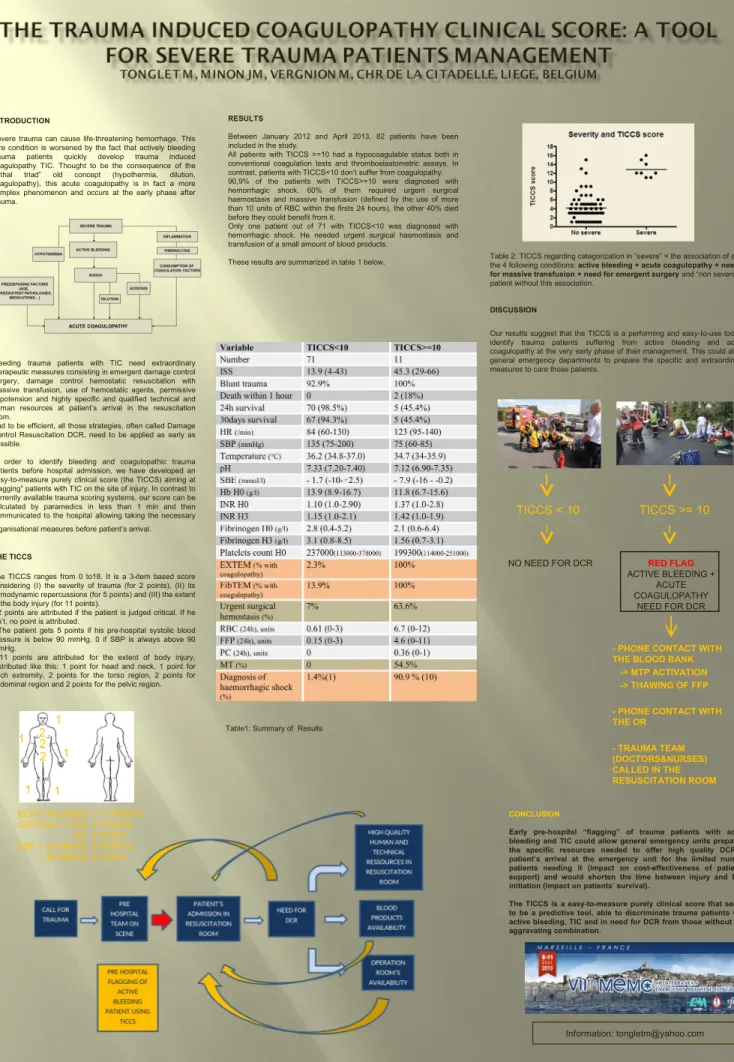
Table 2: TICCS regarding categorization in “severe” = the association of all the 4 following conditions: active bleeding + acute coagulopathy + need for massive transfusion + need for emergent surgery and “non severe” = patient without this association.
DISCUSSION
Our results suggest that the TICCS is a performing and easy-to-use tool to identify trauma patients suffering from active bleeding and acute coagulopathy at the very early phase of their management. This could allow general emergency departments to prepare the specific and extraordinary measures to care those patients.
CONCLUSION
Early pre-hospital “flagging” of trauma patients with active bleeding and TIC could allow general emergency units preparing the specific resources needed to offer high quality DCR at patient’s arrival at the emergency unit for the limited number patients needing it (impact on cost-effectiveness of patient’s support) and would shorten the time between injury and DCR initiation (impact on patients’ survival).
The TICCS is a easy-to-measure purely clinical score that seems to be a predictive tool, able to discriminate trauma patients with active bleeding, TIC and in need for DCR from those without this aggravating combination.
Information: tongletm@yahoo.com
RESULTS
Between January 2012 and April 2013, 82 patients have been included in the study.
All patients with TICCS >=10 had a hypocoagulable status both in conventional coagulation tests and thromboelastometric assays. In contrast, patients with TICCS<10 don’t suffer from coagulopathy. 90,9% of the patients with TICCS>=10 were diagnosed with hemorrhagic shock. 60% of them required urgent surgical haemostasis and massive transfusion (defined by the use of more than 10 units of RBC within the firsts 24 hours), the other 40% died before they could benefit from it.
Only one patient out of 71 with TICCS<10 was diagnosed with hemorrhagic shock. He needed urgent surgical haemostasis and transfusion of a small amount of blood products.
These results are summarized in table 1 below.