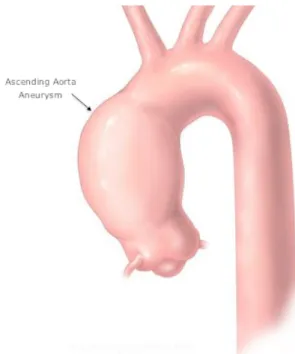
Ascending Aorta Parametric Modeling and Fluid Dynamics Analysis in a Child Patient with Congenital BAV and Ascending Aorta Aneurysm
123
0
0
Texte intégral
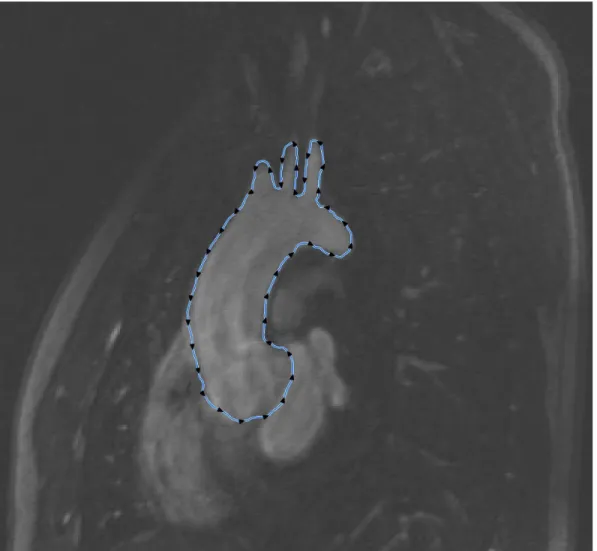
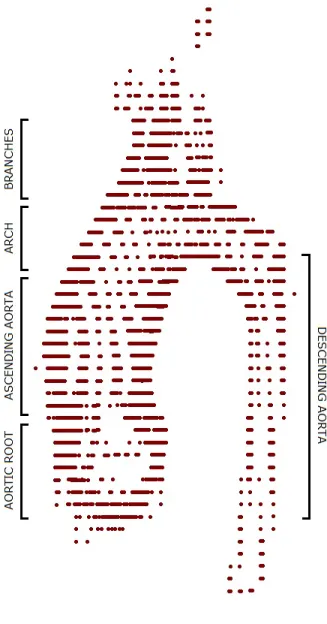
Figure

+7



Documents relatifs
