O
pen
A
rchive
T
OULOUSE
A
rchive
O
uverte (
OATAO
)
OATAO is an open access repository that collects the work of Toulouse researchers and
makes it freely available over the web where possible.
This is an author-deposited version published in :
http://oatao.univ-toulouse.fr/
Eprints ID : 13100
To link to this article :
DOI:10.1016/j.irbm.2014.02.008
URL :
http://dx.doi.org/10.1016/j.irbm.2014.02.008
To cite this version :
Bastide, Rémi and Bardy, Pierre and Borrel,
Bernard and Boszodi, Catherine and Bouet, Marinette and Gani, Kahina
and Gayraud, Eric and Gourc, Didier and Lamine, Elyes and Marenq,
Pierre-Henri and Schneider, Michel and Toumani, Farouk Plas'O'Soins :
a software platform for modeling, planning and monitoring homecare
activities. (2014) IRBM, vol. 35 (n° 2). pp. 82-87. ISSN 1959-0318
Any correspondance concerning this service should be sent to the repository
administrator:
staff-oatao@listes-diff.inp-toulouse.fr
Plas’O’Soins:
A
software
platform
for
modeling,
planning
and
monitoring
homecare
activities
R.
Bastide
a,∗,
P.
Bardy
b,
B.
Borrel
c,
C.
Boszodi
d,
M.
Bouet
e,
K.
Gani
e,
E.
Gayraud
f,
D.
Gourc
g,
E.
Lamine
a,
P.-H.
Manenq
h,
M.
Schneider
e,
F.
Toumani
eaISIS-IRIT,UniversitédeToulouse,CampusUniversitaire,rueFirmin-Oulès,81104Castres,France bUMT,202,avenuePélissier,81100Albi,France
cCentrehospitalierd’Albi,81000Albi,France dCARMI,2,avenueBouloc-Torcatis,81400Carmaux,France
eLIMOS,UniversitéClermont-FerrandII,campusdesCézeaux,63173Aubière,France fCGXSYSTEM,LeCausse,81100Castres,France
gCGI-EMAC,routedeTeillet,81013Albi,France hAlmerys,5,avenueMarcel-Dassault,31500Toulouse,France
Abstract
Demographicchangesinrecentyearshavecontributedtoashiftincaremodels,withthedevelopmentofhomecareasanewalternativeto traditionalhospitalization.Wepresentasoftwareplatformdedicatedtothemodeling,planningandmonitoringofhomecareworkflows,developed intheframeworkoftheFrenchresearchprogramTecSan.Theplatformisusedonthedesktopbycarecoordinators,andonthegobycareworkers usingmobiledevices.
1. Introduction
Francenowcounts14millionpeopleoverage60,so21%of thepopulation.Peopleover75represent8.6%ofthepopulation. Accordingtoestimates,theirnumberwillalmostdoubleinthe next10years.Increasedlifeexpectancyleadstoamorethan pro-portionalincreaseofthe‘fragile’persons.Directconsequence ofthisfindingistheincreasedcostofcareandhospitalization. Thesedemographicchanges,witharapidageingofthe popu-lationandagrowingsegmentofpeoplewithchronicillnesses andphysicaldisabilities,inadditiontotheincreasingcostsin thehealthcaresector,arehavingagrowingandprofoundimpact onthehealthcaresystem[1].Thesechangesleadtoaneedfor newcaredeliverymechanismsandstructures[2].
Out of that, in many countries have come different alternatives. One of thesenewinitiatives is the homecare.In recentyearswearenotinganincreasingdemandforhomecare
∗Correspondingauthor.
E-mailaddresses:Remi.Bastide@irit.fr,Remi.Bastide@gmail.com
(R.Bastide).
services:inFrance,asitismentionedin[3],between2005and 2009thenumberofpersonsunderhomecareincreasedby120%, thenumberofhospitalizationdaysinhomecareraisedby119% and the number of patients increased 148%.In Canada too, homecareorganizationsaregrowingrapidly.Itiseventhemost rapidlyexpandingsectoroftheCanadian healthcaredelivery system[4].
Finding ways to deliver high quality health care adapted tothe needsof thesepatients is amajorchallenge for health caresystem. In response to thischallenge, thereis a consid-erableinternationalinterest inexploitingthe Information and Communication Technologies (ICT)solutions toenhance the qualityandsafety of healthcare ingeneral andhomecare in particular.
Thesetrendsarestrongincentivesfore-Healthresearch.The EuropeanUnionhasundertakenanumberofresearchprojects toassisttheelderly,proposingsolutionstotheissuesof mobil-ity(I2HOME),communication(SHARE-it),remotemonitoring (CAALYX,eCAALYX),timelyaccesstopatientspecific infor-mation(COGKNOW,EasyLine+),andinvolvingpatientsmore activelyintheirowncareprocess(Coplintho).
1.1. TheFrenchhomecareecosystem
InFrance,homecareismainlymanagedbyregional associ-ations,whichcoordinatetheactivityofallthepersonsinvolved (doctors,nurses,housecleaning,mealdelivery,etc.).
Thestakeholdersinthe homecareprocess widelydifferin termsoftheirorganizationalstructure,responsibilityand tech-nicalability:
• most of the medical staff involved in homecare in France (doctors,nurses)areself-employed(liberalprofession):they havenohierarchicdependencyontheorganizationthat man-agestheoverallhomecareprocess.Theyusuallypossesstheir owninformationsystemsupport(albeitverylimited):agenda management,paperordigitalpatientrecords,etc.;
• ontheotherhand,housecleaningandmealdeliveryis usu-ally performed by staff employed by municipalitiesor the homecare association themselves. Thesepeople have little computer literacy,andare oftenreluctanttouse computer-basedsystemintheirdailywork;
• the elderly’s relative oftenlivefar away fromtheir elderly parent, paying him irregular visits. However, they wish to keepintouchwiththeirparent usingphone,andtobekept informedonhishealthstate;
• finally, the homecare system is funded by regional public units,whicharebilledfortheworkofthevarious stakehol-ders.Theseunitsneedtobereliablyinformedoftheactual work that has been performed, timespent athome by the variousstakeholders,etc.
Currently,theactivityofallthesepersonsismanagedlargely manually,usingaso-called‘liaisonlogbook’,aphysical note-bookkeptattheelderly’shome,whichisreadfromandwritten tobyallthepersonsthatinterveneinthepatient’scare, includ-ingthepatient’srelatives.Theliaisonlogbookisgenerallyan unstructured, physical notebook that is kept at the elderly’s home. It is used for communication between the family and thevariousstakeholders.Eachstakeholdernotesthedateofthe visit,theoperationsperformed,recommendationsoranyother formofcomment.
Itisnoteworthythattheliaisonlogbookcontainsveryuseful data,underusedinthehomecareprocess.Indeed,itstores infor-mation of different types: logistical informationwhich helps forthecoordinationofactivities,medicalinformation,general information on the patient, any informationwhich may help improvethequalityofthehomecareandpossiblythedetection ofthepatienthealthchangeviaanintelligentmonitoringsystem.
Thismodeofcommunicationhasseverallimits:
• a communicationthat is not always clearand reliable:the stakeholdersmustscanthroughtheliaisonlogbookfor infor-mationwhichisintendedtothem,orforwhichtheyarelikely tobeinterested.Aslongastheliaisonlogbookremainsatthe patient’shome,thestakeholdersmustnotforgettoreaditand mustbeabletoaccuratelytranscribeitsinformation; • lackofprivacyandsecurity:becausetheliaisonlogbookis
athomeofthedependentperson,eachpartymayhaveaccess
toall informationwritten on the logbook.It canbe easily pollutedwithwronginformation,eitherinadvertentlyorby maliciouspeople.
1.2. Processesinhomecare
The activityof homecaregives risetocommunicationand coordinationproblems.Toensurethecoordinationand continu-ityofcare,andtoimproveitsquality,thecaregiversinvolvedon homecarearemandatedto:
• ensuretheaccuracyofinformation,byautomatingthe trans-missionofinformationandbyavoidingseveraltranscriptions forthesameinformation;
• guaranteethetimelytransmissionofinformationtothe appro-priate stakeholders, be it information about the patient’s conditionorotherlogisticalinformation;
• ensurethetransmissionofinformationabouttheactual medi-calorparamedicalinterventionsperformedbythecaregivers; • ensure the storage of information about the evolution of
patient’shealthconditions.
1.3. Homecareprocesses
Intheliterature,therearemanyresearchworksabout home-care processes andparticularly on medical homecare. In [3], the“Nationalfederationofinstitutionshospitalizationathome” (FNEHAD) provides a mapping process for patients under medical homecare,considering that computer support is still underdevelopedininstitutionsofmedicalhomecare.Thiswork aimstostructureinformationsystemsforhomecareandstands asareferenceinthisarea,asitencompassesallprocesses pre-sentedinotherworks.Fig.1showsthemainprocessesinvolved inhomecare,followingISO9000thatclassifiesprocessesinto threetypes:management,operational(managementofpatient) andsupport(Humanresources,purchasingandlogistics...).
The Plas’O’Soins platform is mainly concerned with the “delivery ofcare”and“coordinationandmonitoring ofcare” processes,whilebeinginteroperablewiththetoolsthatsupport theotherprocesses,suchas“billing”or“humanresources”.
1.4. Workflowinhomecare
Tocopewiththedrawbacksaddressedabove,wesuggestthe automationofsomeprocessesofpatientmanagement.
Wedistinguishtwosets of processes:the firstsetincludes the “admission request”, “preadmission”, “billing stays”and “discharge” processes, which are prone to be automated by a classicalworkflow management system. The second set of processes includes “delivery of care”and “coordination and monitoringofcare”thatarethemaintopicofthepresentpaper. Thecharacteristicsoftheseprocessesmakethedesignof work-flowsfortheirautomationadifficulttask.
Fig.1. Mainprocessesofhomecare.
• itusuallyextendsoverlongperiodsoftime,especiallyinthe caseofchronicillness;
• itrequiresthecoordinationofnumerousanddifferent stake-holders;
• it is non-routine, each patient being aspecificcase dueto particular health conditions,social networking,geographic location,etc.;
• it representsacollaborative process,deployedina dynam-ically evolving setting. The homecare processes present a strong humancomponent,distributedamongseveralactors withvariouslevelsofautonomy;
• itevolvesdynamically,accordingtothechanginghealthofthe patientandhisenvironment.Ingeneral,theprocessitrequired toquicklyandeasilyadapttoachangingenvironment; • it presentsatemporalcomplexity,asthetasksinhomecare
have complex frequency and duration constraints that are inconvenienttorepresentinconventionalworkflowmodels.
Thisorganizationalcomplexityformedtherationaleforthe Plas’O’Soinsproject, describedinthispaper. Thegoalof the projectistodevelopatechnologicalplatformallowingforthe orchestrationofhomecareprocesses,withtheaimtoimprove thistypeofcareandtofaceunforeseenevents.Thisplatformis meanttoanswertheneedsofhomecareorhomehospitalization structures,intermsofcoordination,planningandmonitoringof thecareplans,andofthestakeholders’activities.
ThePlas’O’Soinsplatformprovidesfor:
• the rendering of real-time state of the care process, either globallyoroneper-actorbasis;
• the timely transmission of information (alerts, schedule changes...)towardstheappropriatestakeholder;
• theplanningandcoordinationofactivities,andtheirdynamic re-planning;
• themanagingofcoherenceandtraceabilityofactivities; • thehelptothedecisionprocessbyprovidingstatisticdata.
Plas’O’Soinsdealswiththecoordinationofactivitiesinhome healthcare,activity tracing andmonitoring. The project will provide a platform supporting the definition and agile moni-toringofpersonalizedcareprocesses,helpingtocoordinateand planactivities,whilehelpingthecommunicationbetweenactors, andprovidingefficiencyindicators.
2. Material/Patients
ThePlas’O’Soinsplatformisdesignedtobeusedmainlyby themedical andparamedicalstaff involvedinhomecare.The patients’useoftheplatformmainlyconsistsinconsultingtheir weeklyplanning,andbeinginformedof relevantinformation, suchasthere-schedulingofaplannednursevisit.
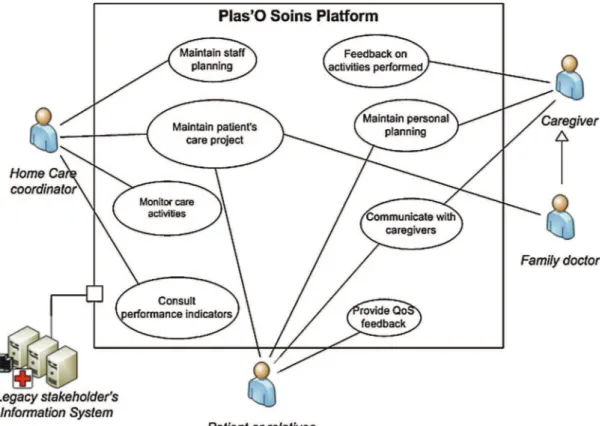
Themainactors/usecasesoftheplatformareasfollows: • homecare coordinator: usually a nurse, employed by the
homecareassociation.Hermainusecasesconsistin: ◦ definingthepatients’careplans,andupdatingthem
accord-ingtotheevolutionofthepatient’shealthstate,
◦ defineorganizationalconstraintsthatareinfluentialtothe schedulingresults,suchasworkingourandperiodicstaff leaves,
Fig.2.UsecasesofthePlas’O’Soinsplatform.
◦ monitortheexecutionofhomecareacts:fromthereal-time informationprovidedbycaregivers,thecoordinatorcanbe informedaboutdelaysintheperformanceofacts; • caregivers(nurses,medicalaids...)usetheplatform“onthe
go”throughsmartphonesorothermobiledevices:
◦ they can access their schedule planning, with the detail of thepatients theyneed tovisitandthemedical actsto performateachpatient’s,
◦ as theyprovidethecare,theycaninformthecoordinator abouttheperformanceandtimelinessoftheactsperformed (Fig.2).
3. Methods
Plas’O’Soinsfeaturesseveralinnovativeaspects,regarding ontheonehandtheinter-organizationalcoordinationbetween stakeholders,presenting awidevariety ininformationsystem support.Ontheotherhandthesystemtacklesthedynamicity ofactivities,resultingfromthemobilityofactors,andfromthe needforpersonalizationofcareprocesses.Plas’O’Soinstackles theconstraintsstemmingforthesensitivenatureofthe informa-tion,anddealwithusabilityandsocialacceptabilityconcerns.
Themainscientificaspectsincludedintheprojectare:
• the definition of a Domain Specific Language (DSL) for homecareprocesses,targetedtoend-userprogramming; • thedefinitionofanagilemediationarchitecturebasedonweb
services,allowingfortheagileexecutionandmonitoringof theprocessesdefinedbytheDSL;
• thedefinitionofaprocessforactivitycontinuity,thatallows ensuringthecontinuingprovidingofcareevenundertechnical andorganizationalfailure.
4. Results
4.1. Adomainspecificlanguageforcareprocesses
Afterathoroughdomainanalysisperformedwithend-users we defined a Domain Specific Language (DSL) for speci-fying care plans. This DSL allows for specifying planned actions,interventionsandthreevisionsofthecareplan(forecast, planned,executed).
A care planis expressedas set of medical and paramedi-calacts(e.g.injection,ortoilet),eachassociatedwithtemporal modalities. Several acts canbe combined intoa single inter-ventioniftheyrequirethesamemedicalexpertise,andiftheir temporalmodalitiesarecompatible.Theexpressionof tempo-rality for acts and interventions,which is an integral part of the DSL, has beenthe subject of aspecificstudy that led to the proposal of a specification language for almost periodic recurrences.
Theobjectiveistoprovidealanguageforexpressing repe-titionsforactsorinterventionsovertimeinacondensedform, similar tothe form used by physicians to their requirements (e.g.“dailyandnightlyfor 3daysandthendailyfor5days”). Acondensedformispreferredbecause itismorecompactto communicatethanadevelopedformsuchasanagendawiththe listofoccurrencesoftheactivity.InadditiontheDSLmustbe abletohandleirregularities.
Table1
Examplesoftemporalexpressions.
Period Days Intervals
Apr.21,2013–May5,2013 Monday,
Wednesday, Friday
Morning,evening
Period Days Intervals
Apr.21,2013–May15,2013 Everyday Morning
Table2
Non-overlappingtemporalexpressions.
Period Days Intervals
Apr.21,2013–May15,2013 Monday,
Wednesday, Friday
Morning,evening
Apr.21,2013–May15,2013 Sunday Morning
ThissectionintroducestheDSLinaintuitivemanner con-sistentwithauser-centeredvision.Amoreformalpresentation isavailablein[5].
Temporality for actsis specified viaa triplet(period,day, intervals). Itis used toexpressasimple regularrepetition as showninthetwoexamplesbelow(Table1).
Daysandintervalscantakedifferentformstoaccommodate variouspossibilitiesencounteredinthemedicalworld.Dayscan bealistofweekdays,oralistofdates,oranexpression(Every day,Everyoddday...).Intervalsmayspecifydailytime-frames (morning,evening...)timeslots(10a.m.–11a.m.)oraspecific time(10a.m.).Allthesevaluesarecombined,providedthatthe correspondingtimeslotsdonotoverlap.
However,arepetition ofactsisnotalwaysentirely consis-tent.Inadditiontheremaybeexceptions.Ourlanguageallows combining several specifications of temporality to express a superpositionofpatternsorexceptions.
Thiscombinationisnotaproblemaslongasthedays asso-ciatedwithvariousexpressionsarepairwisedisjointedasinthe followingexample(Table2).
However, aproblemarises when the days associated with different expressions are not disjointas shownbelow. In the followingexample,thereisambiguitybecausewedonotknow if Sundayactivity must takeplaceinthe morningandin the eveningorinthemorningonly(Table3).
Toresolvethisambiguity,weintroducethenotionof over-load:astatementoverloadsallthoseprecedingit.Sointheabove examplethesecondtermisthefirstpriorityforeverySunday.
With thisnotionof overloadit iseasytoexpresscomplex repetitionsor exceptions,byinsertingasmanyexpressionsas needed andrankingthemproperly.In theexample below,the
Table3
Overlappingtemporalexpressions.
Period Days Intervals
Apr.21,2013–May15,2013 Everyday Morning,evening
Apr.21,2013–May5,2013 Sunday Morning
Table4
Overloadedtemporalexpressions.
Period Days Intervals
Apr.21,2013–May15,2013 Everyday Morning,evening
Apr.21,2013–May15,2013 Sunday Morning
Apr.21,2013–May15,2013 Holiday None
activityoccurseverymorningandevening(general),excepton Sundayswhen it occurs onlyin the morning(specificity). In caseofholiday,theactivityisnotmaintained(otherspecificity) (Table4).
From the condensed representation, we can produce an expandedformsuitableforanagendabyprocessingeachline, startingfromthelastone.
4.2. Planningstrategies
Theconceptofinterventionisusedtodescribeavisitatthe patient’shome,undertakenby amedical or paramedicalstaff onaspecifiedtimeslot.Theremaybeoneorseveraltechnical actsperformedbythestaffonasinglevisit.Thiscombinationof actsmayberequiredandscheduledbythecoordinatorfor tech-nicalreasons,and/orproposedbythecareplaneditorsoftware. Interventionsarecomposedofaspecificidentifier,thepatient involved,thespecifiedtimeof care,thedayscheduledforthe interventionandthedesiredtimerange.
Asoftwaremoduleisdedicatedtocalculateafeasible plan-ningofall therequiredinterventions,taking intoaccount the availabilityof medical orparamedical staff[6].The planning modulealsoconsidersthegeo-localizationofpatients,inorder tominimizethedrivingdistancerequiredtovisitallthepatients daily.Theplanningmoduleshastheresponsibilitytoorganize allplannedinterventionsintoshifts,i.e.aseriesofinterventions thatcanbeperformedbyasinglestaffmemberinasingleday, takingintoaccounttheworkinghoursandthedrivingdistance involved.
Thenumberofshiftsperdayandtheiramplitudearerequired inordertobuildtheschedules.Everypossibleshiftis character-izedbythestarttimeandendtimetocomplywith,thetypeof feasibleinterventionsdependingontheworkerassignedtothe shift.
Planninghastodetermineastarttimeforeachintervention considered,andtoinsertitintoashift.Theplanningalgorithm aimstooptimize,whilerespectingcertainconstraints,thetravel timebetweenpatientsforallactstobeperformedononeday.
Theplanningmoduleusesavariantofthetabusearch algo-rithm[7]toconstructsasetofsolutionsthatmeettheconstraints set.Thesesolutionsarevisuallypresentedtotheuser,whocan select the preferred solution. It may happen that no solution canbe providedthat complieswiththe constraint.This situa-tionisnotexceptional,andinthiscasethecoordinatorhasthe opportunitytohirenewself-employednurses,andthusrelaxthe constraintsontheavailableworkforce.
Toevaluatethesolutionsprovidedbytheplanningmodule, wehavedefinedseveralcriteria tocompare andseekthebest
solutions.Thesecriteriaweredevelopedbasedondiscussions withend-users.
• timewindows,thiscriterionensuresthattheplanned interven-tionsinthissolutionarewellplannedinaccordancewiththe desiredtimeslots.Avalueofzeroindicatesthatalloperations complywiththeconstraints,whileapositivevalueindicates thetotalamountofoverflowsininterventions;
• durationoftheshift;
• timebetweeninterventions:Inthecaseofmultiplevisitsto the samepatient duringasingle day, itis requested that a minimumperiod(e.g.3hours)isobservedbetweeneachvisit soastospreadoverthewholeday.
5. Discussion
Theconstraint-basedplanningapproachpresentsapotential flaw: it is quite common that all relevant constraints are not formallyexpressed,eitherbecausethesoftwaredoesnotallow forit,orbecausethecoordinatorwouldbereluctanttoexpress constraints of intimate nature (such as, for instance, the fact thattherearepersonalconflictsbetweenanurseandapatient). Asaresult,theresultsoftheschedulingalgorithmmayprove unsatisfactory.
Toalleviateforthisconstraint,weallowthecoordinatorto choose from the solutions provided by the algorithm,and to manuallyadjustschedules,aslongastheinitialconstraintsare met.Theschedulingforthepastweekisalsofedasaninputto thealgorithm,whichwillfavorsolutionswithminimal disrup-tionsfrompreviousschedules.Webelievethatthisstrategywill producesatisfactoryschedules,eventhoughallconstraintsare notformallyexpressed.
ThecaregiversaccessthePlas’O’Soinsplatformonthego, through mobile devices such as smartphones or tablets. Cur-rently, the care staff has little computer literacy, and is not accustomedtotheuseofmobiledevices.Withtheend-users part-nersinthePlas’O’Soinsconsortium,wehaverunexperiments ofthemobileuserinterfacewiththecarestaff,inrealistic situa-tions.Severalproblemshavebeenpointedout,someresulting fromlackofpracticewithmobiledevices,andothersresulting
fromtechnicalandethicalquestioningfromthestaff,such as thefearofbeingcontinuouslytrackedbythesystemduringtheir workingshift.Theseusabilityconcernsneedtobetackled,and achangeleadingstrategyhastobedefinedtoensureasmooth integrationofthisnewtechnologywithinthecurrentpractices andhabitsofhomecare.
6. Conclusion
Theworkpresentedherehasbeendevelopedinthe frame-workofprojectPlas’O’Soins,anationwideprojectfundedbythe French NationalAgencyforResearch(ANR),withinthe Tec-SanframeworkandisalsosupportedbytheCancerBioSanté cluster.
The Plas’O’Soins consortium includes academics, ICT industries and end-users. Associated partners contribute to projectmanagement,ethicsandlawconcernsandalsorepresent theagenciesthatfundhomehealthcareinFrance.
References
[1]BastideR,ZefouniS,LamineE.InformationSystemArchitecturefor Home-CareWorkflowManagement.TheInternationaleHealth,Telemedicineand HealthICTForumforEducation,NetworkingandBusiness(Med-e-Tel), 14/04/2010-16/04/2010.Luxembourg:National ChengKung University; 2010[electronicmedium].
[2]BoulosK,MagedLN,CastellotR,AnastasiouA,NugentCD, Alexan-derssonJ,etal.Connectivityforhealthcareandwell-beingmanagement: examplesfromsix Europeanprojects.Int JEnvironResPublicHealth 2009;6(7):1947–71.
[3]FNEHAD.Livreblandessystèmesd’informationenhospitalisationà domi-cile;2009.
[4]LewisS,DonaldsonC,MittonC,CurrieG.Thefutureofhealthcarein Canada.BMJ2001;323(7318):926–9.
[5]BouetM,GaniK,SchneiderM,ToumaniF.Ageneralmodelforspecifying nearperiodicrecurrentactivities-applicationtohomecareactivities.2013 IEEE15thInternationalConferenceone-HealthNetworking,Applications andServices(Healthcom2013).IEEE;2013.p.207–11.
[6]GourcD,MarmierF.Towardsanalgorithmforhomecarescheduling. Work-shopOptimisationdesSystèmes,AméliorationContinueetTransformation desEntreprises;2013.
[7]BurkeE,DeCausmaeckerP,VandenBergheG.AhybridTabusearch algo-rithmforthenurserosteringproblem.SecondAsia-PacificConferenceon SimulatedEvolutionandLearning;1998.p.187–94.