HAL Id: dumas-01903536
https://dumas.ccsd.cnrs.fr/dumas-01903536
Submitted on 24 Oct 2018HAL is a multi-disciplinary open access archive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come from teaching and research institutions in France or abroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, est destinée au dépôt et à la diffusion de documents scientifiques de niveau recherche, publiés ou non, émanant des établissements d’enseignement et de recherche français ou étrangers, des laboratoires publics ou privés.
Distributed under a Creative Commons Attribution - NonCommercial - NoDerivatives| 4.0 International License
FDPM study : a back and forward translation of
multimorbidity in German, Bulgarian, Bosnian, Croat,
French, Polish, Greek and Italian
Charles Rivet
To cite this version:
Charles Rivet. FDPM study : a back and forward translation of multimorbidity in German, Bulgarian, Bosnian, Croat, French, Polish, Greek and Italian. Life Sciences [q-bio]. 2014. �dumas-01903536�
1
UNIVERSITÉ de BRETAGNE OCCIDENTALE
FACULTÉ DE MÉDECINE
ANNÉE 2014 N°
THÈSE D'EXERCICE
Pour le
DOCTORAT DE MÉDECINE
DE SPÉCIALITÉ MÉDECINE GÉNÉRALE
Par
Mr RIVET Charles
Né le 12 Mai 1986, à Grasse (Alpes Maritimes)
PRÉSENTÉE ET SOUTENUE PUBLIQUEMENT LE 12 Juin 2014
FDPM study: A back and forward translation of multimorbidity
in German, Bulgarian, Bosnian, Croat, French, Polish, Greek and
Italian.
Président : Professeur J-Y. LE RESTE Membres du Jury :
Professeur J-Y. LE RESTE Professeur C. BERTHOU Docteur P. NABBE Docteur C. LIETARD
2
UNIVERSITE DE BRETAGNE OCCIDENTALE
FACULTE DE MÉDECINE ET
DES SCIENCES DE LA SANTÉ DE BREST
PROFESSEURS EMÉRITES
Professeur BARRA Jean-Aubert Chirurgie Thoracique & Cardiovasculaire Professeur LAZARTIGUES Alain Pédopsychiatrie
DOYENS HONORAIRES: Professeur H. H. FLOCH
Professeur G. LE MENN ()
Professeur B. SENECAIL
Professeur J. M. BOLES
Professeur Y. BIZAIS ()
Professeur M. DE BRAEKELEER
3
PROFESSEURSDES UNIVERSITÉSEN SURNOMBRE
Professeur BLANC Jean-Jacques Cardiologie Professeur CENAC Arnaud Médecine Interne
PROFESSEURSDES UNIVERSITÉS - PRATICIENS HOSPITALIERSDE CLASSE EXCEPTIONNELLE
BOLES Jean-Michel Réanimation Médicale
FEREC Claude Génétique
GARRE Michel Maladies Infectieuses - Maladies tropicales
MOTTIER Dominique Thérapeutique
PROFESSEURSDES UNIVERSITÉS - PRATICIENS HOSPITALIERSDE 1ère CLASSE
ABGRALL Jean-François Hématologie - Transfusion
BOSCHAT Jacques Cardiologie & Maladies Vasculaires
BRESSOLLETTE Luc Médecine Vasculaire
COCHENER - LAMARD Béatrice Ophtalmologie
COLLET Michel Gynécologie - Obstétrique
DE PARSCAU DU PLESSIX Loïc Pédiatrie
DE BRAEKELEER Marc Génétique
DEWITTE Jean-Dominique Médecine & Santé au Travail
FENOLL Bertrand Chirurgie Infantile
4
JOUQUAN Jean Médecine Interne
KERLAN Véronique Endocrinologie, Diabète & maladies métaboliques
LEFEVRE Christian Anatomie
LEJEUNE Benoist Epidémiologie, Economie de la santé & de la prévention LEHN Pierre Biologie Cellulaire
LEROYER Christophe Pneumologie
LE MEUR Yannick Néphrologie
LE NEN Dominique Chirurgie Orthopédique et Traumatologique
LOZAC’H Patrick Chirurgie Digestive
MANSOURATI Jacques Cardiologie
OZIER Yves Anesthésiologie et Réanimation Chirurgicale
REMY-NERIS Olivier Médecine Physique et Réadaptation ROBASZKIEWICZ Michel Gastroentérologie - Hépatologie
SENECAIL Bernard Anatomie
SIZUN Jacques Pédiatrie
TILLY - GENTRIC Armelle Gériatrie & biologie du vieillissement
PROFESSEURSDES UNIVERSITÉS - PRATICIENS HOSPITALIERSDE 2ème CLASSE
BAIL Jean-Pierre Chirurgie Digestive
BERTHOU Christian Hématologie – Transfusion
BEZON Eric Chirurgie thoracique et cardiovasculaire
5
BOTBOL Michel Psychiatrie Infantile
CARRE Jean-Luc Biochimie et Biologie moléculaire
COUTURAUD Francis Pneumologie
DAM HIEU Phong Neurochirurgie
DEHNI Nidal Chirurgie Générale
DELARUE Jacques Nutrition
DEVAUCHELLE-PENSEC Valérie Rhumatologie
DUBRANA Frédéric Chirurgie Orthopédique et Traumatologique
FOURNIER Georges Urologie
GILARD Martine Cardiologie
GIROUX-METGES Marie-Agnès Physiologie
HU Weigo Chirurgie plastique, reconstructrice et esthétique ; brûlologie
LACUT Karine Thérapeutique
LE GAL Grégoire Médecine interne
LE MARECHAL Cédric Génétique
L’HER Erwan Réanimation Médicale
MARIANOWSKI Rémi Oto. Rhino. Laryngologie
MISERY Laurent Dermatologie - Vénérologie
NEVEZ Gilles Parasitologie et Mycologie
NONENT Michel Radiologie & Imagerie médicale NOUSBAUM Jean-Baptiste Gastroentérologie - Hépatologie PAYAN Christopher Bactériologie – Virologie; Hygiène
6
RENAUDINEAU Yves Immunologie
RICHE Christian Pharmacologie fondamentale
SALAUN Pierre-Yves Biophysique et Médecine Nucléaire
SARAUX Alain Rhumatologie
STINDEL Eric Bio-statistiques, Informatique Médicale et technologies
de communication
TIMSIT Serge Neurologie
VALERI Antoine Urologie
WALTER Michel Psychiatrie d'Adultes
PROFESSEURS des Universités – praticien Libéral
LE RESTE Jean Yves Médecine Générale
PROFESSEURS ASSOCIÉS
LE FLOC'H Bernard Médecine Générale
MAITRES DE CONFERENCESDES UNIVERSITÉS - PRATICIENS HOSPITALIERS HORSCLASSE
ABALAIN-COLLOC Marie Louise Bactériologie – Virologie ; Hygiène
AMET Yolande Biochimie et Biologie moléculaire
LE MEVEL Jean Claude Physiologie
LUCAS Danièle Biochimie et Biologie moléculaire
RATANASAVANH Damrong Pharmacologie fondamentale
7
MAITRES DE CONFERENCESDES UNIVERSITÉS - PRATICIENS HOSPITALIERSDE 1ère CLASSE
ABALAIN Jean-Hervé Biochimie et Biologie moléculaire
AMICE Jean Cytologie et Histologie
CHEZE-LE REST Catherine Biophysique et Médecine nucléaire DOUET-GUILBERT Nathalie Génétique
JAMIN Christophe Immunologie
MIALON Philippe Physiologie
MOREL Frédéric Médecine & biologie du développement et de la reproduction
PERSON Hervé Anatomie
PLEE-GAUTIER Emmanuelle Biochimie et Biologie Moléculaire
UGO Valérie Hématologie, transfusion
VALLET Sophie Bactériologie – Virologie ; Hygiène
VOLANT Alain Anatomie et Cytologie Pathologiques
MAITRES DE CONFERENCESDES UNIVERSITÉS - PRATICIENS HOSPITALIERSDE 2ère CLASSE
DELLUC Aurélien Médecine interne
DE VRIES Philine Chirurgie infantile
HILLION Sophie Immunologie
LE BERRE Rozenn Maladies infectieuses-Maladies tropicales
LE GAC Gérald Génétique
LODDE Brice Médecine et santé au travail
8
SEIZEUR Romuald Anatomie-Neurochirurgie
MAITRESDECONFERENCES-CHAIREINSERM
MIGNEN Olivier Physiologie
MAITRES DE CONFERENCES
AMOUROUX Rémy Psychologie
HAXAIRE Claudie Sociologie - Démographie
LANCIEN Frédéric Physiologie
LE CORRE Rozenn Biologie cellulaire
MONTIER Tristan Biochimie et biologie moléculaire
MORIN Vincent Electronique et Informatique
MAITRESDECONFERENCESASSOCIESMI-TEMPS
BARRAINE Pierre Médecine Générale
NABBE Patrice Médecine Générale
CHIRON Benoît Médecine Générale
AGREGES DU SECOND DEGRE
MONOT Alain Français
9
Résumé :
Introduction : L’OMS définit la multimorbidité par l’atteinte d’au moins deux états de
maladies chroniques chez une personne. Toutefois le mot « état » n’est pas suffisamment explicite pour une utilisation pratique de cette définition. Le EGPRN (European General Practice Research Network) qui s’engage dans l’étude des concepts autour des soins primaires en médecine générale a défini la multimorbidité à l’aide d’une revue systématique de la littérature. Une traduction de la définition semble indispensable pour être employée à travers l’Europe. L’objectif de cette étude est de voir si une traduction aller-retour couplée à une méthode Delphi permet d’obtenir un consensus sur la définition de la multimorbidité. De plus une analyse méta-ethnographique a contrôlé l’homogénéité des définitions.
Méthode : L’étude a formé huit équipes d’experts européens en utilisant l’aide de l’EGPRN.
Une première traduction allée fut élaborée à l’aide d’un traducteur officiel et de deux chercheurs en médecine générale. L’étude a ensuite soumis cette définition aux différents experts en utilisant une méthode Delphi pour déterminer un consensus sur la définition. Finalement la définition retour a bénéficié d’une analyse méta-ethnographique pour vérifier la conservation d’homogénéité par rapport à la définition allée.
Résultats : L’étude a inclus deux cent dix sept experts représentant huit pays Européens.
Tous les résultats ont été représentés dans des tableaux.
Discussion : Le problème posé par la traduction de concepts n’est pas nouveau en recherche
médicale. Plusieurs techniques sont utilisées dont la méthode de traduction aller-retour qui assure l’homogénéité des concepts d’une culture à l’autre. Cette étude a permis d’obtenir un consensus et de valider la définition de la multimorbidité à travers huit pays Européens. L’analyse méta-ethnographique a confirmé l’homogénéité des définitions et permet leur utilisation en recherche de soins primaires.
10
Summary:
Background: Multimordity is defined by the World Health Organization (WHO) as a person
being affected by two or more chronic conditions. However, the world “condition” is not sufficiently clear for practical purpose and leads to misinterpretations. The European General Practice Research Network (EGPRN) is committed to concepts in primary care and defined multimorbidity using a systematic review of literature. To help European researchers model and restructure health care centered on patients; a translation had to be conducted. The intention of this study is to see if consensus is obtained using a back and forward translation combined with a Delphi analysis within European experts. Furthermore, the study did a meta-ethnographic analysis to inspect homogeneity.
Method: Using experts selected with EGPRN the study formed eight multilingual teams. A
forward translation was defined using one official translator and at least two general practitioner researchers. The study used a Delphi methodology to determinate consensus among the included experts. Meta-ethnography analysis was performed on the backward definitions.
Results: The study gathered two hundred and seventeen experts representing eight European
countries. All results were transcribed into tables and then analyzed.
Discussion: The problem of translation is not new in the field of medicine. Different
techniques are used, including back and forward method that insures homogeneity with concept from one culture to another. This study has validated the definition of multimorbidity in eight European languages. The meta-ethnographic analysis confirmed homogeneity for each definition.
11
Table of Contents :
1. Introduction:
122. Method:
143. Results:
164. Discussion:
204.1 Results summary 20
4.2 Similar studies involving translation in the field of medicine. 21
4.3 Limits: 24
5. Conclusion:
256. Bibliography:
2712
1-Introduction :
Multimorbidity was first published in Germany in 1976 (1). The concept began its
internalization in 1990 through research (2) and was an addition to the concept of comorbidity which was defined as any disease or risk factors that could interact with one main disease with the effect of making it worst. Multimorbidity added an overview of all factors that could lead to frailty (3-4-5).
Multimordity is defined by the World Health Organization (WHO) as a person being affected by two or more chronic conditions (6). WHO’s intention was to look at all conditions in one individual that could impact on that individual’s global health status.
However, the world “condition” is not sufficiently clear for practical purpose and leads to misinterpretations.
The European General Practice Research Network (EGPRN) is committed to concepts that are able to advance research in primary care throughout Europe (7). The EGPRN national teams did a systematic review of literature using multimorbidity as Keyword. Searched data bases were Pubmed, Embase and Cochrane. For inclusion, multimorbidity criteria were described in the article. For results EGPRN had 416 founded abstracts, 68 selected abstracts, 54 included articles and 1631 founded criteria of definition.
Criteria’s were arranged in 11 thematic codes. The selective coding achieved the following definition: Multimorbidity is defined as any combination of chronic disease with at least another disease (acute or chronic) or a bio psychosocial factor (associated or not) or a risk factor. Any bio psychosocial factor, any risk factor, the social network, the burden of disease, the health care consumption and the patient’s coping strategies may function as modifiers. Multimorbidity can modify the health outcomes and lead to an increased disability or decreased quality of life or frailty (8).
13
The Multimorbidity definition is extremely close to family medicine core competencies. It seems also informative for long-term care given the increasing prevalence of chronic illness in an ageing population across Europe and all developed countries. It can help researchers in family medicine investigate the complexity of patient’s conditions and their overall impact on patient health and is an additional tool to identify frail patients with the intention of
preventing illness (9).
In order to help European researchers and medical team’s model and restructure health care centered on patients, a translation of this exhaustive definition into all the languages within the teams had to be conducted (10).
Because the Delphi method is an iterative process to collect and distill the anonymous judgments of experts using a series of data collection and analysis techniques interspersed with feedback. This method works especially well when the goal is to improve our
understanding of problems. The Delphi method has its origins in the American business community, and has since been widely accepted throughout the world in many sectors including health care. It is a method for structuring a group communication process to facilitate group problem solving and to structure models (11).
Validating a definition needs an ethnographic perspective; Bruno Latour’s work invites to conceive translation as a production process that relies on intermediaries operating in networks. Hence, the translated text does no longer appear as the “simple” reflection of the norms of a given society or that of the subjectivity of the translator, but rather as the expression of the relations between the various intermediaries that have participated in its production (12).
The intention of this study is to see if consensus is obtained for the definition of
14
European teams. Furthermore, the team completed the study by a meta-ethnographic analysis to see if homogeneity was obtained.
2-Method:
The study started forming multilingual teams representing eight nationalities (Bosnia, Bulgaria, Croatia, France, Germany, Greece, Italy and Poland). Each participant had to meet four “expertise” requirements to be included in our study: The knowledge and experience with general practice and multimorbidity, the capacity and willingness to participate,
sufficient time to participate and sufficient English level for effective communication. Experts were selected using the help of EGPRN. The study gathered information about the expert’s gender, age, years of practice, English level and publication quotas. Signed testimonies were obtained from each participant to insure inclusion criteria. Each team had to be formed by at least ten experts.
The study began making samples at the end of year 2012. The final validation of this study occurred during spring 2013 and a meta-ethnographic analysis was performed during Mai 2013.
A forward translation was defined using one official translator and at least two general practitioner researchers. The team isolated key words which were analyzed to define
concepts. The study pointed out two key words: “bio-psychosocial factors” and “risk factors” which needed clarification. The forward definition was then emailed to all experts.
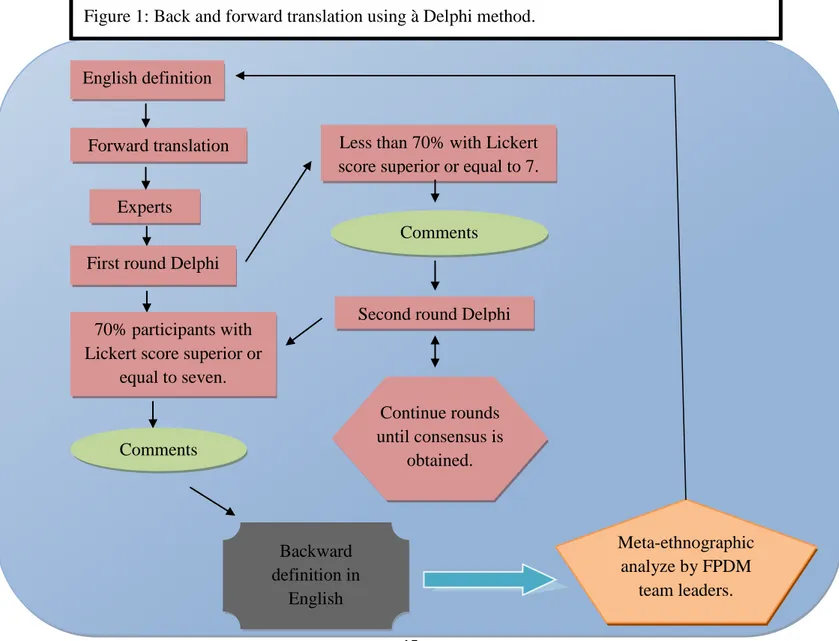
The study used a Delphi methodology to determinate the extent to which consensus existed among the included experts. Consensus took place in a series of “rounds”. The first round entailed, the study obtained the opinions of included experts about the multimorbidity definition in there spoken languages. In subsequent rounds the same experts were asked to rate the extent of their agreement or disagreement with a series of statements describing the
15
opinions expressed in the first round. Responses were analyzed for the degree of consensus achieved. Failure to reach consensus resulted in further rounds. The study assured anonymity of Delphi participants allowing participants to freely express their opinions without undue social pressures to conform from others in the group. The translation obtained consensus when at least seventy percent of scores were superior or equal to seven, on a scale of nine (The Lickert scale). If consensus was not obtained a new translation was proposed using remarks from participants. When consensus was obtained the backward translation was submitted to the original authors for final validation. (Fig 1).
Finally a meta-ethnography analysis was performed by the leaders of FDPM on the backward definitions to confirm homogeneity between original and final definition.
English definition
Forward translation
Experts
First round Delphi
70% participants with Lickert score superior or
equal to seven.
Comments
Backward definition in
English
Less than 70% with Lickert score superior or equal to 7.
Comments
Second round Delphi
Continue rounds until consensus is obtained. Meta-ethnographic analyze by FPDM team leaders. Figure 1: Back and forward translation using à Delphi method.
16
3-Results:
The study gathered two hundred and seventeen experts representing eight European countries. (Table 1) Country Gender Average Age in years Average years of practice English Level Average English publications Other publications Total
N=217 M F Read Spoken Written
1 Bosnia N=14 5 9 43,29 16,71 x x x 2,79 8,43 2 Bulgaria N=30 11 19 47,03 21,8 x x x 0,27 1 3 Croatia N=22 3 19 50,14 23,36 x x x 14,68 36,36 4 France N=30 18 12 47,43 19,17 x x x 3,23 16,57 5 Germany N=31* 19 12 54,48 19,76 x x x 9,33 24,9 6 Greece N=30 18 12 45,67 12,63 x x x 10,2 61,22 7 Italy N=30 19 11 50,7 24,17 x x x 4,38 19 8 Poland N=30 15 15 43,67 12,2 x x x 1,75 6,27 Global Average (%) 49,77 50,23 47,80 18,73 100% 5,83 21,72
*German averages were calculated using twenty one experts who had answered the study with complete
information. The study conserved all the thirty one participants for Lickert scores in order to limit data loss in Delphi rounds procedures.
17 Country Numbers of
Delphi rounds
Mean consensus score for final turn
Numbers of comments for all
rounds Bosnia 2 7,9 27 Bulgaria 1 8,2 6 Croatia 1 8,5 9 France 2 7,4 64 Germany 2 7,8 18 Greece 1 8,3 9 Italy 1 7,6 10 Poland 1 7,56 6 Mean for Europe 1,375 7,908 18,625
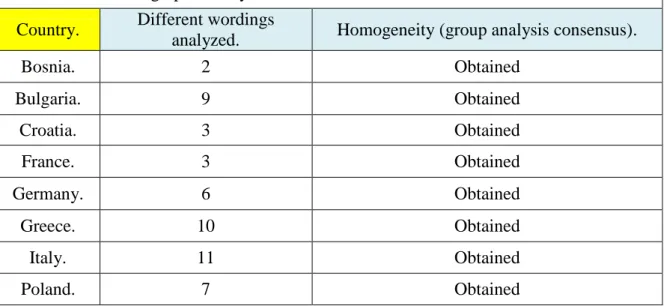
Homogeneity was compared with the backward translation by applying a meta-ethnographic analysis. (Table 3)
Table 3: Meta-ethnographic analysis. Country. Different wordings
analyzed. Homogeneity (group analysis consensus).
Bosnia. 2 Obtained Bulgaria. 9 Obtained Croatia. 3 Obtained France. 3 Obtained Germany. 6 Obtained Greece. 10 Obtained Italy. 11 Obtained Poland. 7 Obtained
18
English original Bosnia Bulgaria France
Multimorbidity is defined as any combination of chronic disease with
at least one other disease (acute or chronic) or bio-psychosocial factor (associated or not) or somatic risk factor. Any bio-psychosocial factor,
any somatic risk factor, the social network, the burden
of diseases, the health care consumption and the
patient’s coping strategies may
function as modifiers (of the
effects of Multimorbidity).
Multimorbidity may modify the health outcomes and lead
to an increased disability or a decreased quality of
life or frailty.
Multimorbidnost(pacijent sa više bolesti u isto vrijeme) je definisana kao svaka kombinacija bolesti sa najmanje još
jednom nekom bolešću(akutnom ili
hroničnom) ili bio-psihosocijalnim faktorom
koji je udružen ili ne) ili somatskim faktorom rizika. Svaki bio-psiho-socijalni faktor,svaki faktor rizika,socijalna podrška,raširenost bolesti,korištenje zdravstvene zaštite i
način kako se sam pacijent nosi sa bolešću,može dovesti do promjene.(efekata multimorbidnosti). Multimorbidnost-višebolesnost može mijenjati ishode zdravlja
i voditi povećanoj nesposobnosti ili sniženom kvalitetu života
ili povećanoj osjetljivosti. Полиморбидност се определя като всяка комбинация от хронично заболяване, с поне едно друго заболяване (остро или хронично) или свързан или не със заболяването био-психо-социален фактор или друг соматичен рисков фактор. Всеки био-психо-социален фактор, всеки рисков фактор, социалната среда, тежестта на заболяванията, използването на здравни услуги и стратегии на пациента за справяне могат да оказват влияние върху ефектите на полиморбидността. Полиморбидността може да доведе до промяна на очакваните резултати и до по-висока степен на инвалидност, понижено качество на живот или слабост. La multimorbidité est définie comme toute combinaison
d’une maladie chronique avec au
moins : une autre maladie (aiguë ou chronique) ou un facteur biopsychosocial (associé ou non) ou un facteur de risque somatique. Les effets de la multimorbidité peuvent être modifiés par : tout
facteur biopsychosocial, tout facteur de risque somatique, le réseau social, le poids des maladies, la consommation de soins de santé et les stratégies adaptatives du patient. La multimorbidité
peut modifier les résultats de santé et mener à une augmentation du handicap ou à une diminution de la qualité de vie ou à la fragilité. » Table 4: English Original and final translation for each country.
19
Germany Greece Italy Poland
Definiert als jegliche Kombination einer chronischen Erkrankung
mit zumindest einer weiteren Erkrankung (akut oder chronisch), oder einem
bio-psycho-sozialen Faktor(assoziiert oder
nicht) oder einem somatischen Risikofaktor. Jeglicher bio-psycho-soziale Faktor, jeglicher Risikofaktor, das soziale
Netzwerk, die Krankheitslast, die Inanspruchnahme des Gesundheitssystems sowie persönliche Bewältigungsstrategien können die Auswirkungen von Multimorbidität beeinflussen. Multimorbidität kann Gesundheitsparameter beeinflussen und Funktionseinbußen verstärken. Sie kann auch die Lebensqualität
reduzieren oder zu Gebrechlichkeit führen Ως πολυνοσσηρότητα ορίζεται κάθε συνδιασμός οξέων ή χρόνιων νοσημάτων με ή χωρίς συσχετιζόμενους ή μη συσχετιζόμενους βιοψυχοκοινωνικούς παράγοντες ή σωματικούς παράγοντες κινδύνου. Αυτοί οι παράγοντες μπορούν επίσης να λειτουργήσουν ως τροποποιητές, παράλληλα με τον κοινωνικό ιστό, τη χρήση υπηρεσιών υγείας και τις στρατηγικές αντιμετώπισης του ασθενούς. Μπορεί να τροποποιήσει τα αποτελέσματα στην υγεία και να οδηγήσει σε μια αυξημένη ανικανότητα, μια μειωμένη ποιότητα ζωής ή ευθραστότητα. Si definisce multimorbidità ogni combinazione di una malattia cronica con almeno un’altra
malattia (acuta o cronica), o un fattore bio-psicosociale (associato o meno), o un fattore di rischio somatico. Ogni fattore bio-psicosociale, ogni
fattore di rischio somatico, la rete sociale, il carico delle malattie, l’uso dei servizi sanitari e le strategie con cui i pazienti affrontano i loro problemi possono fungere da agenti modificanti (degli effetti di multimorbidità). La multimorbidità può modificare i risultati di salute e portare ad un incremento della disabilità o ad un peggioramento della qualità della vita o a
fragilità. Wielochorobowość jest definiowana jako jakiekolwiek połączenie choroby przewlekłej z przynajmniej jeszcze
jedną chorobą (ostrą lub przewlekłą) lub
z czynnikami bio-psycho-społecznymi
(związanymi z nią lub nie) lub z czynnikami ryzyka. Jakikolwiek czynnik bio-psycho-społeczny, czynnik ryzyka, sieć społeczna, obciążenie chorobami, korzystanie z opieki zdrowotnej i strategie radzenia sobie przez pacjenta mogą funkcjonować jako modyfikatory. Wielochorobowość może modyfikować wyniki zdrowotne i prowadzić do zwiększonej niepełnosprawności lub obniżenia jakości życia lub
20
4-Discussion:
4.1-Results summary:
The study gathered two hundred and seventeen experts around multimorbidity definition within eight European countries. It took an average of 1.375 rounds to obtain consensus. France, Germany and Bosnia obtained consensus in two rounds, their comments were used to modify the initial definition and elaborate a new one for the second round Delphi. More generally all comments were noted (even if consensus was obtained in one round) enabling to see concepts that had met difficulties with translation.
The studies meta-ethnographic analysis confirmed homogeneity between each backward translation and the initial translation. The team found a more affirmative posture in German and Greek who ignore conditional in there spoken languages. Italians linguistic posture was gentler; this reflected the state of mind of Italian GPs. The patients coping strategies were differently appreciated in post communist countries (Bosnia, Bulgaria, Poland and Croatia) but also in Bosnia’s Muslim culture were the Muslim determinism is opposed to the free will of the western society. Post communist countries added social infrastructures to the social network considered as family and friends in the western society. Phrases were turned upside down for adjectives and verbs in most continental languages without losing sense.
The concept of frailty met difficulties in translation reflecting the lack of knowledge behind this concept.
21
4.2-Similar studies involving translation in the field of medicine:
The team searched other medical articles whose goals were the translation of medical concepts to demonstrate the importance of sharing acute information in order to obtain a better and more global approach of patients within different ethological groups. It also helped compare different techniques that had been used.
For example, the Mini mental state examination (MMSE) test is a practical test used for evaluating cognitive status. A study showed that many experts in France use this test to include patients in studies or start specific treatment. One of the major problems in using the MMSE in French version compared to the American original version is the translation of concepts. This implies that subjects may be included because they have the same score but not the same symptoms. A rough translation could induce different socio-cultural meanings, modify the difficulty of the test and induce the inclusion of patients who are defined as similar but in reality are not. For orientation in time and space the MMSE requests the name of “town, country and state” this implied translation difficulties because the administrative division of the United States of America is different than the administrative organization in France. Finally the words maintained in French had to be adapted to French “culture” and had to be able to answer one main question: can a taxi driver find the address with the words used. The chapter of repetition and remembering in the MMSE test uses three words that must not be close in semantics or phonetics. The words are to have the same length and frequencies for a given language. This made the literal translation into French impossible and a new series had to be elaborated. (13).
Likewise, the orientation items (“season” and “state) have specific local,
geographical/political referents pertinent to the United States, possibly rendering a
22
of the contributing factors to item bias in cognitive measurements for example the MMSE-item “no ifs, ands or buts” has been found consistently to be easier for Latino than for non-Latino respondents and for those who are tested in Spanish as contrasted by English. A possible explanation for this finding is that the translation of this item in some of Spanish versions of the MMSE does not reflect the actual intent of the original English item. Language translation and transfer across cultures can have an impact on psychometric properties of a test by affecting the difficulty of the test. The process used in instrument translations should ensure that original and translated measures are both conceptually equivalent as well as cross culturally valid. Differences in item content may affect comparisons across studies and interpretations of findings. The use of different idiomatic expressions or even of totally different content (that still hold the intent of the original items) may be an appropriate approach to pursue “measurement equivalence” even within
populations with a shared language. (15)
Another study aiming to test and measure the properties of the French translation of the Disease Burden Morbidity Assessment (DBMA) was translated using cognitive interviews and obtained similar properties in median, sensitivity and specificity. It performed a test-retest that showed high test reliability. The DBMA being a self-report questionnaire used to
estimate the disease burden experienced by patients, this definition made it possible to work with same concepts in French and English (original version). (16)
Equally, the French translation of the Patient Scar Assessment Scale (PSAS) is used to measure patient’s satisfaction related to scarring after orthopedic surgery. It was carried out by a Canadian team using a forward and backward translation. The French version was successfully translated and demonstrated strong psychometric properties. The PSAS is now a tool used for English speaking patients for evaluation of scars which can also be used in French. (17)
23
Evenly, the Substance Use Risk Profile Scale (SURPS) has been developed to screen risk factors for substance misuse. This scale assesses four high-risk personality traits using a twenty three item, self-report questionnaire. SURPS helps guiding targeted approaches to prevention of substance abuse and misuse. It has been validated in the United Kingdom, English Canada, Sri Lanka and China. A Quebec study validated this scale in a sample of French-speaking adolescents from Quebec as well as its sensitivity in clinical sample of adolescents. The final aim of the study was targeting Quebec adolescents to include them in a national prevention program, PREVENTURE. (18)
As well, the four item index of the nineteen item Acne Quality of life (Acne-Qof) has been validated in English. A French translation and linguistic validation of the Acne-Qol has recently been completed. This study sought to evaluate reliability and responsitivity of the French version using calculation of intraclass correlation coefficients and regression modeling. In the end the abbreviated Acne-QoL in French was somewhat reflective of the entire Acne-QoL and by its brevity facilitated psychometric evaluation of francophone acne patients in routine practice. (19)
Also, the WOSI (Western Ontario Shoulder Instability Index) is a self-administrated quality of life questionnaire designed to be used as a primary outcome measure in clinical trials on shoulder instability, as well as to measure the effect of an intervention on any particular patient. It is validated and is reliable and sensitive. A study aimed to produce a French language version of the WOSI culturally adapted to both European and North American French speaking populations. Reliability and responsiveness analyses were carried out. A French version was accepted by a multinational committee and was then validated using a total of one hundred and forty four native French-speaking subjects from Canada and Switzerland. The creation of this questionnaire aims to facilitate outcome assessment in French-speaking settings. (20)
24
Finally the “Parkinson Neuro-psychometric Dementia Assessment” (PANDA) is a convenient tool, validated in German, to assess cognition in Parkinson disease. It consists of five
cognitive tasks and a brief mood questionnaire, and is designed for the early detection of mild cognitive deficits as well as dementia. The study translated PANDA into French and provided normative data for a French speaking population. The translation was made by means of the translation/re-translation method. Statistics were conducted with SPSS Statistics 18. The results indicated that the PANDA French translation could be used with the same
transformation algorithms as the German version, when adding a correction for the education. (21)
4.3-Limits:
Selection bias:
They were limited by the inclusion procedure of experts. The expert’s English level was appreciated using a questionnaire making us sure they were capable of reading and speaking English. The study included thirty one German experts that answered the Delphi round obtaining consensus in two rounds; unfortunately the means calculated for population characteristics used twenty one experts due to the lack of complete response from German experts. Information missing was either gender, age and years of practice.
Information bias:
The study had no information bias since the initial definition was the same and given to every participants answering the Delphi procedure.
Confounder:
Some experts had not published in English even though English level was acceptable for each expert. The study used Delphi scores of all thirty one German experts event thought the
25
means of characteristic was calculated using twenty one experts; this was done to exploit maximum sample size with Germans in order to give a larger impact in consensus.
Bosnia added a fifteenth expert in the Delphi round calculation which seemed to be
transcription error. After checking with Bosnia we confirmed that only fourteen experts had been selected for that country and we removed the fifteenth Delphi score from our calculation.
Sample characteristics:
Groups of experts were chosen with the help of the EGPRN network. Anonymous requests were asked from experts to verify their field of knowledge and competencies. The quality of each group is questionable. Not all experts had the same number of publications.
5-Conclusion
:
The problem of translation is not new in the field of medicine. Many studies attempt to translate concepts, tests and definition to apply them on different types of population. The lack of quality in translation can lead to misinterpretation or health impairments.
Different techniques are used including back and forward method using expert’s evaluation to obtain a good quality translation and insure homogeneity with concept from one culture to another.
Up to now international studies using the OMS definition of multimorbidity agreed that the concepts behind this definition were vague. This induced lack of scientific proof and confusion bias due to problems with interpretation and patient inclusion.
This study has validated the EGPRN definition of multimorbidity in eight European
languages using a back and forward translation with a Delphi consensus. The realization of a meta-ethnographic analysis confirmed homogeneity for each translated definition. Even
26
though the concept of frailty stays indecisive the new definition has lifted doubt on the term “condition” from the OMS definition. The EGPRN definition is now usable for research protocols between these European countries.
27
6-Bibliographie:
1. Brandlmeier P. Multimorbidity among elderly patients in an urban general practice. ZFA. Zeitschrift für Allgemeinmedizin. 1976 Sep 10;52(25):1269–75.
2. Heuft G. Future research perspectives of a psychoanalytical gerontopsychophysiology--personality and the aging process. Zeitschrift für Gerontologie. 1990;23(5):262–6. 3. Starfield B. Global health, equity, and primary care. Journal of the American Board of
Family Medicine : JABFM. 2007;20(6):511–3.
4. Beasley JW, Starfield B, Van Weel C, Rosser WW, Haq CL. Global health and primary care research. Journal of the American Board of Family Medicine : JABFM. 2007;20(6):518–26.
5. Boyd CM, Shadmi E, Conwell LJ, Griswold M, Leff B, Brager R, et al. A pilot test of the effect of guided care on the quality of primary care experiences for multimorbid older adults. Journal of general internal medicine. 2008;23(5):536–42.
6. World Health Organization. The World Health Report 2008. primary health Care - Now more than ever. World Health Organization; 2008.
7. Hummers-Pradier E, Beyer M, Chevallier P, et al. Series: the research agenda for general practice/family medicine and primary health care in Europe. Part 4. Results: specific problem solving skills. Eur J Gen Pract 2010;16: 174-181.
8. Le Reste, J., Nabbe, P., Manceau, B., Lygidakis, C., Doerr, C., Lingner, H, Lietard, C. The European General Practice Research Network presents a comprehensive definition of Multimorbidity in Family Medicine and Long-Term Care, following a systematic review of relevant literature. Journal of the American Medical Directors Association 2013;14(5), 319–25.
9. Fried LP, Ferrucci L, Darer J, et al. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol Ser A Biol Sci Med Sci 2004;59:255-263.
10. Le Reste JY, Nabbe P, Lygidakis C, Doerr C, Lingner H, Czachowski S, et al. A Research Group from the European General Practice Research Network (EGPRN) Explores the Concept of Multimorbidity for Further Research into Long-Term Care. J Am Med Dir Assoc 2012;13(7)1-2.
11. Skulmoski GJ, Hartman FT, Krahn J. The Delphi Method for Graduate Research. J Inf Technol Educ. Citeseer; 2007;6(1):1.
12. Buzelin H. La traductologie, l’ethnographie et la production des connaissances. Meta J des traducteurs 2004;49(4):729.
28
13. Derouesné C, Po J, Hugonot L, Kalafat M, Dubois B, Laurent B. Mini-Mental State Examination: a useful method for the evaluation of the cognitive status of patients by the clinician. Presse med 1999;28(21):1141-8.
14. Ramirez M, Teresi JA, Holmes D. Differential Item Functioning (DIF) and the Mini-Mental State Examination (MMSE) Overview, Sample, and Issues of Translation. Med Care. 2006;44(11):95–106.
15. Poitras M-E, Fortin M, Hudon C, Haggerty J, Almirall J. Validation of the disease burden morbidity assessment by self-report in a French-speaking population. BMC Health Serv Res 2012;12:35-42.
16. Rouleau DM, Alami G, Macdermid JC. Translation of the Patient Scar Assessment Scale ( PSAS ) to French with cross-cultural adaptation. Can J Sur 2009;52(6):259–63. 17. Castonguay-jolin L, Perrier-ménal-d DE, Castellanos-ryah N, Parent S, Vitaro F,
Tremblay RE, et al. SURPS French version validation in a Quebec adolescent population. Can J Psychiatry 2013;58(9):538–45.
18. Tan J, O’Toole A, Zhang X, Dreno B, Poulin Y. Evaluation of the French version of the 4-item index of the Acne-QoL (AcneQ4fr). Qual Life Res 2013;22(3):547–9. 19. Gaudelli C, Balg F, Godbout V, Pelet S, Djahangiri a, Griffin S, et al. Validity,
reliability and responsiveness of the French language translation of the Western Ontario Shoulder Instability Index (WOSI). Orthop Traumatol Surg Res Elsevier Masson SAS 2014;100(1):99–103.
20. Gasser A-I, Kalbe E, Calabrese P, Kessler J, Von Allmen G, Rossier P. French translation and normation of the Parkinson Neuropsychometric Dementia Assessment (PANDA). J Neurol Sci Elsevier B.V. 2011;310(1-2):189–93.
Annexes:
Analyse méta-ethnographique: cf. CD
29
RIVET Charles – FDPM study: A back and forward translation of multimorbidity in German, Bulgarian, Bosnian, Croat, French, Polish, Greek and Italian.
Thèse. : Médecine. : Brest 2014 ABSTRACT:
Background: Multimordity is defined by the World Health Organization (WHO) as a person being affected by two or more chronic conditions. However, the world “condition” is not sufficiently clear for practical purpose and leads to misinterpretations. The European General Practice Research Network (EGPRN) is committed to concepts in primary care and defined multimorbidity using a systematic review of literature. To help European researchers and model and restructure health care centered on patients; a translation had to be conducted. The intention of this study is to see if consensus is obtained using a back and forward translation combined with a Delphi analysis within European experts. Furthermore, the study did a meta-ethnographic analysis to inspect homogeneity.
Method: Using experts selected with EGPRN the study formed eight multilingual teams. A forward translation was defined using one official translator and at least two general practitioner researchers. The study used a Delphi methodology to determinate consensus among the included experts. Meta-ethnography analysis was performed on the backward definitions.
Results: The study gathered two hundred and seventeen experts representing eight European countries. All results were transcribed into tables and then analyzed.
Discussion: The problem of translation is not new in the field of medicine. Different techniques are used, including back and forward method that insure homogeneity with concept from one culture to another. This study has validated the definition of multimorbidity in eight European languages. The meta-ethnographic analysis confirmed homogeneity for each definition.
MOTS CLES :
MULTIMORBIDITY ; FAMILY MEDICINE ;
JURY : Président : Professeur J-Y. LE RESTE
Membres Professeur J-Y. LE RESTE, Professeur C. BERTHOU, Docteur P. NABBE, Docteur C. LIETARD
DATE DE SOUTENANCE : Jeudi 12 juin 2014