ORGANIZATIONAL DYNAMICS OF SUPPORTED EMPLOYMENT PROGRAMS FOR PEOPLE WITH SEVERE MENTAL ILLNESS
Mémoire présenté
à la Faculté des études supérieures de l'Université Laval dans le cadre du programme de maîtrise en santé communautaire
pour l'obtention du grade de maître ès sciences (M.Sc.)
DÉPARTEMENT DE MÉDECINE SOCIALE ET PRÉVENTIVE FACULTÉ DE MÉDECINE
UNIVERSITÉ LAVAL QUÉBEC
2009
La présente étude qualitative visait à mieux comprendre l'influence des dynamiques organisationnelles sur l'implantation des programmes de soutien à l'emploi (SE) pour personnes atteintes de problèmes de santé mentale graves au Québec. Les résultats démontrent la présence de deux coalitions en lien avec ces programmes, soit une reliée au secteur de la santé et une reliée au secteur de l'emploi. La vision qui chapeaute les services des acteurs de la santé en est une de rétablissement et leurs services adhèrent ·généralement aux principes du modèle «Individual Placement and Support». Comme ces acteurs, les acteurs de la coalition d'emploi visent aussi l'intégration de leurs clients en emplois compétitifs. Par contre, leurs valeurs et croyances différentes et la nature de leurs partenariats influencent ces derniers
à
organiser leurs services différemment des acteurs de la santé. Ensemble, les deux formes de SE semblent répondre aux besoins variés des utilisateurs de services vocationnels.This qualitative study aimed to beUer understand how the organizational dynamics between àctors has influenced the implementation and functioning of supported employment (SE) programs for people with severe mental illness living in the province of Quebec. Two main coalitions of actors related to SE programs were identified; one consisting primarily of actors in the health sector and another comprising mainly employment sector actors. Health coalition actors organized their services around the concepts of rehabilitation and recovery and promoted the delivery of SE services consistent with the individual placement and support mode!. Though employment coalition actors also aimed to facilitate their clients' integration into competitive employment, the SE services they provided were different because of important differences in the nature of their relationships and in their values and beliefs. Results suggest that both forms of SE respond to needs in the population and that accessibility to both types should be improved.
Working on this project has been a great joy and a tremendous learning experience. 1 am extremely grateful to the many people who contributed and were involved in the project, as weil as those who have provided me with their love, support and encouragement.
Over the course of this study, 1 was fortunate enough to meet many extraordinary individuals who have devoted their careers to helping others ~scape exclusion and integrate into society. Whether they were service providers, managers or decision makers, their courage, dedication and passion has truly been an inspiration to me. The experiences and points of view that they shared with me through their participation have helped me gain a greater appreciation of the goals they strive for and the challenges that they face. 1 sincerely thank them for their kindness, their amazing generosity and their boundless efforts.
1 am also indebted to the fellow members of my research lab, who welcomed me so warmly two years ago and whose support has never wavered since that time. Many of them went out of their way to ensure that 1 felt comfortable and integrated in the lab, and 1 feel very blessed to have been surrounded by individuals like that. 1 would especially like to thank Élisabeth Martin, my wonderful office-mate, for her friendship and guidance, as weil as Nathalie Houle, the best coordinator a research team could hope to have, for her frequent assistance, optimism and enthusiastic support. Finally, the possibil.ity of working with Daniel Reinharz was one of the driving factors behind my decision to move to Quebec and 1 am tremendously grateful for the opportunity he has provided me, as weil as the limitless kindness and faith he has shown in me. Thank you for your encouragement and for sharing your vast expertise with me.
1 have also been privileged to be part of a larger research team that featured some of the most competent and renowned researchers from across the country. By way of their curiosity, the depth of their expertise and willingness to implicate themselves, these individuals have been able to make a positive difference in the lives of many people.
who have been dynamic leaders and whose determination have been vital to the project's success. My own involvement in the project was also facilitated by the financial support of the Fonds de la recherche en santé du Québec (FRSQ), and 1 thank them for making this experience possible.
Finally, 1 would like to express my most profound thanks to my family and friends for the love and support they have always provided me. 1 would not be where 1 am today without you. To my son, Noah, thank you for being the most wonderful baby boy a father could have. And to my beautiful, amazing wife Amélie, you have been my greatest supporter and my greatest inspiration. So much of this would not have been possible without you. Thank you for ail thé sacrifices you have made for me. 1 love you, and 1 share this achievement with you.
Résumé
---
II
III
Summary
---Foreword
---
IV
L~tofFigures_________________________________________________ _
VIII
IXList of Tables
---Annexes
---
X
Introduction
---
1
L
Cu~~s~~~knowk~e________________________________ _
4
1.1. The role of work and its value as a tool for social integration ___________ _ 4 1.2. Mental illness and work in Canada: a historical perspective ___________ ~ 5 1.2.1. Wo~inilie~y~mcra ________________________________________________ ~ 5 1.2.2. Work in the era of deinstitutionalization and regionalization _______________________ _ 8 1.2.3. The emergence of alternative psychiatrie resources and community-grown vocational ervices 12 1.3.Supported employment ____________________________________________ _ 19 1.3.1. Origins and principles of the supported employment mode} _____________________ _ 19 1.4. Implementation of supported employment in a Canadian context _____________ _ 24
2
R~earcho~ectivesandquestions____________________
__
_________
~28
2.1. ~esearch objectives __________________________________________________ __ 28 2.2 ~esea rch q u estio ns ____________________________________________________ __
293. Methods
30
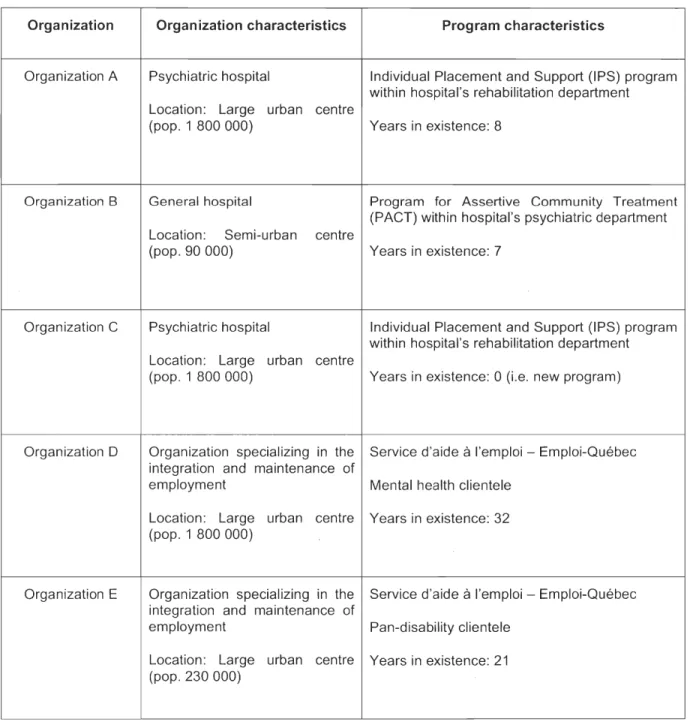
---3.1. An a Iytic a p p roa ch _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ 30 3.2.Sites _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
_
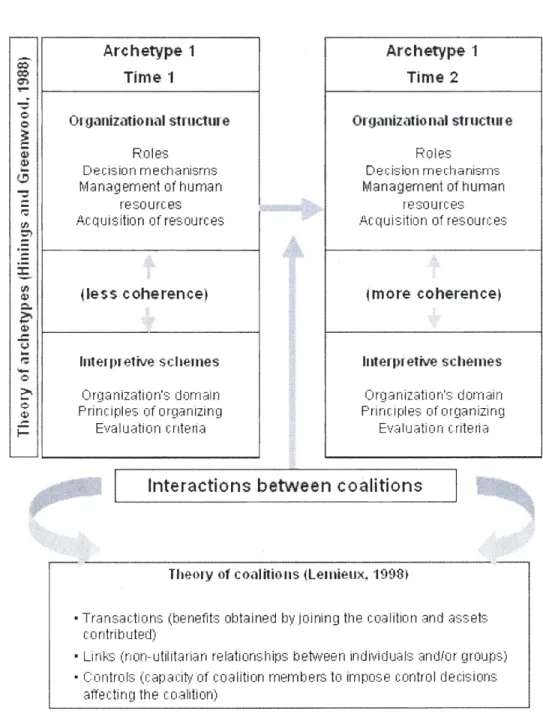
30 3.3." Theoretical frameworks 32 ---3.3.1. Coalition theory ___________________________________________________ _ 32 3.3.2. Hinings and Greenwood's theory ofarchetypes _______________________________ _ 343.4. Data collection 38
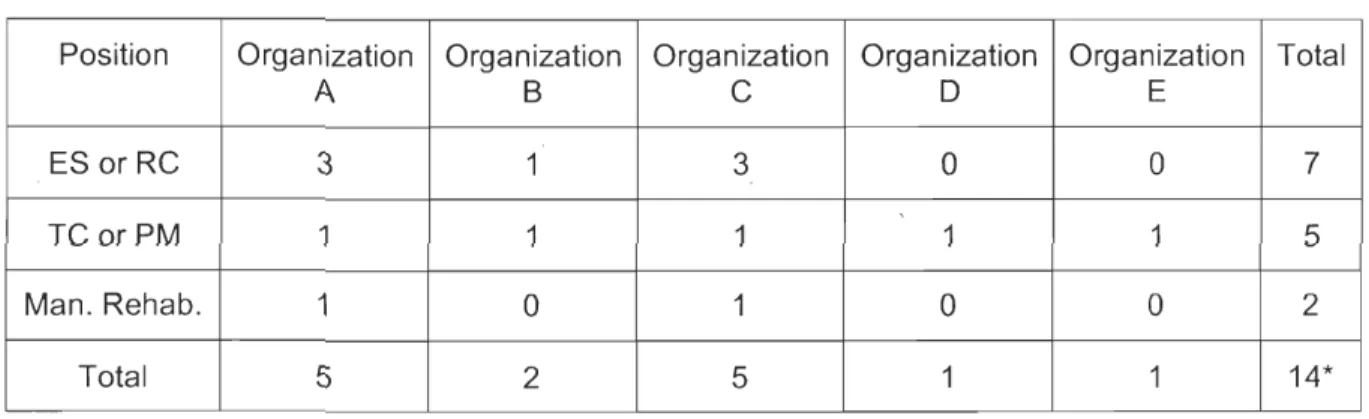
---3.4.1. Sources of information 38 - - - -- - - -- - - -- - - -- - - -3.4.2. ln strumentati on _____________________________________________________ _ 39 3.4.3. ~ata collectionprocedure _____________________________________________ __ 40 3.6. ~alidation ofresults ______________________________________ ~ 43 3.7. ~thicalconsiderations ________________________________________________ __
434.1. Health sector coalition 46
4.1.1. Coalition actors and objectives 46
4.1.2. Transactions 46
4.1.3. Links 52
4.1.4. Controls 57
4.1.5. Archetypes - Organizational structure 61
4.1.6. Archetypes - Interpretive schemes 68
4.1.7. Coherence between organizational structure and interpretive schemes 74
4.2. Employment sector coalition 76
4.2.1. Coalition actors and objectives 76
4.2.2. Transactions 76
4.2.3. Links 80
4.2.4. Controls 81
4.2.5. Archetypes - Organizational structure 86
4.2.6. Archetypes - Interpretive schemes 93
4.2.7. Coherence between organizational structure and interpretive schemes 100 4.3. Interactions between coalitions and coherence between archetypes 102
5. Discussion
104
5.1. The implementation of supported employment in Quebec 104
5.2. Recommendations and limitations 113
5.2.]. Recommendations 113
5.2.2. Limitations 115
6. Conclusion
118
Figure 1: Theoretical frameworks used for the study _ _ _ _ _ _ _ _ _ _ __ _ 37
Figure 2: Health sector coalition Annexe 1
Table 1: Characteristics of organizations and SE programs in the study _ _ _ _ _ _ 31 Table 2: Distribution of interviews across the five organizations 42 Table 3: Summary of health coalition characteristics Annex 2 Table 4: Summary of employment coalition characteristics Annex 3
Annex 1: Figures 2 and 3 Annex 2: Table 3
Annex 3: Table 4
Annex 4: Consent Forms
Whether it be directly or indirectly, mental health problems affect ail members of society. They touch men and women of ail ages, education and income levels, and cultural backgrounds. Approximately twenty percent of Canadians will personally experience a mental illness at some point in their lifetimes (Santé Canada, 2002). In addition, at least 2 to 3% of the population will have mental health problems that are considered severe. While there is sometimes debate as to what constitutes a «severe mental illness», mental health problems are generally considered severe when they cause profound distress and significantly hinder an individual's ability to function in one or more domains of their lives (e.g. school, work, social and family interactions) (Santé Canada, 2002; The Standing Senate Committee on Social Affairs Science and Technology, 2004). Further accentuating the detrimental impact that mental illness can have on people's lives is the fact that the onset of most mental illnesses occurs during adolescence and early adulthood, considerably altering the life courses of many young citizens and their families and placing a heavy burden on the health system and society as a whole. Indeed, for many people with severe mental illness, the road to recovery is fraught with challenges and obstacles, challenges and obstacles that many fail to overcome, causing them to plunge downwards to the margins of society.
For many decades now, the plight of people with severe mental illness and their exclusion from society has been a major concern to numerous stakeholders. There is a wide consensus that their reintegration into society is an important goal that benefits not only the individuals touched by mental illness but also their communities and ail of society. Moreover, those directly affected by mental illness have long expressed a desire for an equal access to the fundamental elements of citizenship, including access to housing, educa,tion and employment. Such a desire was famously articulated by renowned consumer-survivor Pat Capponi, who stated that «the needs of members of the psychiatrie community are not so different, really, from anybody else's needs - a home, a job, a friend» (Capponi, 2003). Such sentiments are echoed by Gary Bond, who states that individuals with severe mental illness want to «live, work, play, and lead their daily lives without distinction from and with the same opportunities as individuals without disabilities» (G. R. Bond, Salyers, Rollins, Rapp, & Zipple, 2004).
---ln response to these needs, the last several decades have seen the emergence of a variety of initiatives that have aimed to facilitate this process of social integration. In the area of work, such services range from pre-employment services such as pre-vocational assessment and counselling services, work readiness and skill development programs, volunteer work and transitional employment to employment services such as supported employment, adapted work centres, social enterprises, consumer-run businesses, and self-employment supports. Within this array of vocational. services, supported employment programs have been the type of service that has received the most attention from researchers. According to the scientific literature, these programs yield superior work outcomes than most other vocational approaches, thus helping more people integrate into regular, competitive 1 employment (G. R. Bond, Salyers, Rollins, Rapp, & Zipple, 2004; Cook, Leff et aL, 2005; Crowther, Marshall, Bond, & Huxley, 2001; Twamley, Jeste, & Lehman, 2003). Indeed, the extensive documentation on supported employment and the scientific support for the model has led it to be viewed as an «evidence-based practice» and «best practice» by many researchers, service providers and policy makers (G. R. Bond et aL, 2001; G. R. Bond, Salyers, Rollins, Rapp, & Zipple, 2004; Goldner, 2002).
As the literature on supported employment has grown, so too has the number of supported employment programs. Implementation of the supported employment model has spread from the United States to Canada, Europe, Asia and other parts of the world. Not surprisingly, such widespread implementation efforts have led to questions about the model's generalizability to contexts outside of the US. For example, service providers in Canada operate in a social, political, economic and cultural environment that is different than that found in the US. Aspects such as Canada's socialized health care system, welfare laws, disability regulations and economic landscape seem to have an importa'nt impact on the structure and effectiveness of supported employment programs developed in this country, though to date only a few studies have touched on these issues (Corbière, Bond, Goldner, & Ptasinki, 2005; Latimer & Lecomte, 2002; Latimer et aL, 2006).
1 Competitive employment is generally defined as being a job in the community, paying at least minimum
ln addition to cross-country differences, there are also within-country differences that play a role in shaping supported employment programs. As more research is carried out in Canada, researchers are becoming increasingly aware of the high degree of variability that exists between programs operating in different provinces and even regions (Corbière, Submitted; Mercier, Provost, Denis, & Vincelette, 1999). Indeed, despite the vast literature on supported employment and efforts to regulate its ~mplementation, the key elements of the model remain unequally applied across settings. This variability could be a cause for concern, as the faithful implementation of supported employment has been shown to be positively correlated with vocational outcomes (O. R. Becker, Smith, Tanzman, Drake, & Tremblay, 2001; D. R. Becker, Xie, McHugo, Halliday, & Mar:tinez, 2006). Thus, identifying factors that give rise to this variability is important as a more complete implementation of this evidence-based practice could lead to better vocational outcomes for clients.
One such factor underlying the observed differences between supported employment programs could be that the stakeholders respons.ible for these programs differ in therr values, ideologies, beliefs and philosophies about the best ways to operate their program and address the needs of service users in their communities. Organizations and stakeholders operate in a context where they must interact with a variety of other actors and react to different environmenté;ll incentives and constraints. Understanding the dynamics of these interactions and how they influence these stakeholders' values and beliefs will likely shed some light on why programs are structured and operated differently in different contexts.
Thus, the goal of the present work was to gain a better understanding of the organizational dynamics related to supported employment programs in one Canadian province, the province of Quebec, and learn more about how various factors, including the values of stakeholders and their relationships with others and with their context, impact the implementation of these programs as a whole, as weil as their key components individually.
1. 1. The raIe of work and its value as a tool for social integration
Work represents a significant part of the lives of most people. It is highly valued by society and provides us with a sense of belonging and the feeling that we can contribute to society's goals (Morin, 1996). It allows us to connect with others, build relationships and shape our social identity (Morin, 1996; Stuart, 20'06). Through work, we can gain the respect of others and achieve a greater social status (Anthony & Blanch, 1987; Dorvil,
Guttman, Ricard, & Villeneuve, 1997; Morin, 1996). We can provide for ourselves, build our self-esteem and ensure our security (Dorvil, Guttman, Ricard, & Villeneuve, 1997;
Vézina, Cousineau, Mergler, Vinet, & Laurendeau, 1992). It offers us challenges and can provide us with a sense of accomplishment (Dorvil, Guttman, Ricard, & Villeneuve, 1997;
Morin, 1996). It enables us to feel more in control of our environment and provides us with a sense of empowerment (Dorvil, Guttman, Ricard, & Villeneuve, 1997). Indeed, work is a fundamenta'i element of citizenship, a basic right and a powerful tool for promoting equality and inclusion.
People with severe mental illness have long expressed a desire to work, and more particularly work in regular, competitive employment (McQuilken, Zahnisher, Novak, & aL,
2003; Mueser, Salyers, & Mueser, 2001). Yet, the regular workforce has remained largely inaccessible to them despite a range of services developed to meet their needs. For instance, studies have shown that approximately 80 to 90% of people with severe mental illness wishing to engage in competitive work remain unemp~yed (Anthony & Blanch,
1987; Crowther, Marshall, Bond, & Huxley, 2001; The Standing Senate Committee on Social Affairs Science and Technology, 2006). Furthermore, they have been shown to be three to five times more likely to be unemployed than the general population (Sturm,
Gresenz, Pacula, & Wells, 1999). The social and economic costs that result from this exclusion place a serious burden on individuals and on society, especially when one considers that one in five Canadians will be touched by mental illness in their lifetime (Santé Canada, 2002).
Helping people with severe mental illness integrate the workforce has been, and is still, a major goal for many stakeholders. Indeed, many actors perceive employment to be one of the most privileged routes towards recovery and social integration (Dorvil, Gutlman, Ricard, & Villeneuve, 1997). While a multitude of barriers to work integration exist (Cook, 2006; Leclerc, Bourassa, & Legros, 2008; Marwaha & Johnson, 2004), numerous studies show that people with severe mental illness can integrate the workforce and make positive contributions to society (O. Becker, Whitley, Bailey, & Drake, 2007).
1.2. Mental illness and work in Canada: a historical perspective
While interest in the socio-professional integration of people with mental illness can sometimes seem like a relatively recent phenomenon, a look back into Canadian history shows that work have long been described as an essential aspect of a normal life and, in the case of those directly touched by mental illness, an important contributor to improved mental health. In the following sections, 1 will outline how the relationship between work and mental health has historically been perceived by some actors and how the organization of psychiatrie services in Canada, and more specifically ·in Quebec, has influenced work integration ideologies and services past and present.
1.2.1. Work in the asylum era
The history of psychiatrie services in Canada can generally be divided into two eras. The first era began in the mid to late 1800s with the building of làrge, long-stay psychiatrie hospitals, referred to often as the «asylums» ·(Davis, 2006). At the time, it was thought that the asylums would play an important role in providing «safe settings for physical and spiritual care and to shield residents from the harm and peril that commonly befell people with mental health illnesses in cities and towns» (Santé Canada, 2002, p.1). Indeed, asylums were viewed by many as a medical breakthrough that allowed individuals with mental illness to have access to the most progressive forms of mental health care (Moran & Wright, 2006).
For many asylum operators, work was claimed to be an integral part of their residents' medical and «moral» therapy (Moran & Wright, 2006). As explained by Geoffrey Rheaume, «Physical exercise brought about by certain types of work, such as agricultural
labour or working in a laundry, was viewed as an essential way of redirecting a person's
alienated mind from their troubles onto the task at hand. As weil, doing regular, steady
work would supposedly lead to towards regular, steady, and above ail, rational habits and
away from mad thoughts» (Rheaume, 2006, p. 70). Therapeutic benefits aside, other
factors motivated asylum administrators to encourage asylum residents to work, most
notably the rising costs related to hospital maintenance and expansion. Asylum residents
were often encouraged to participate in a variety of types of labour, though for the most
part their compensation would consist only of the occasional bribe or privilege2 (Moran &
Wright, 2006). Indeed, unpaid patient labour saved administrators and provincial
governments significant amounts of money and undoubtedly contributed to the survival and proliferation of these hospitals. Despite some concerns regarding the exploitation of
patient labourers, the decades that followed saw hospital administrators and staff maintain
the position that work, as opposed to idleness, contributed to the health and well-being of
its patient population (Rheaume, 2006).
ln Quebec, hospital administrators and medical staff were so convinced of work's
importance in terms of health, rehabilitation and social integration that the acquisition of a
regular, paid job became a necessary condition for permanent leave from the hospital
(Pagé, 1961). Residents who had responded weil to treatment and whose condition had
improved could apply to have their recovery recognized by a hospital tribunal consisting of
administrators and clinicians. If the tribunal was satisfied with their recovery, applicants
would receive medical clearance that would make their recovery official. They would then be occasionally allowed to leave the hospital on a temporary basis in order to secure employment in the community. If the applicant was successful in obtaining work and could
provide firm proof of this to the hospital tribunal, a long-term leave was typically granted.
However, those who could not secure employment, despite their official medical clearance,
were not granted their freedom and would have no choice but to remain andwork inside the asylum. As Charbonneau explains, «For the medical and administrative authorities of
that time, the acquisition and guarantee of employment was considered to be among the
determinants of health and well-being. Work was perceived to be an essential part of
social integration, normalization, recovery, and the maintenance and strengthening of mental health» (Charbonneau, 2002).
As time passed however, the optimism that once surrounded the psychiatrie institutions began to dissipate, giving way to a growing sense of insatisfaction with regards to this method of delivering care. Indeed, critics increasingly insisted that very little care was being offered in the asylums and that these had gradually taken on a mere custodial role, in essence becoming hl1ge warehouses for the mentally ill (Davis, 2006; Santé Canada, 2002). Several factors contributed to this insidious shift in roles, including outdated treatment approaches that were largely ineffective, the public, religious and medical community's growing belief that .mental health pro~lems were incurable and hospital funding methods that favoured the intake of patients (Dorvil, Guttman, Ricard, & Villeneuve, 1997; Fleury & Grenier, 2004). As hospital costs continued to rise, administrators' capacity to meet these costs became increasingly difficult, in part because of an aging and less productive population of patient labourers (Moran & Wright, 2006).
ln Quebec, the 1950s saw the arrivai of a new breed of psychiatrist, one that had been trained in the United-States or in France and who had witnessed the emergence of new medications and mental health reform (Dorvil, Guttman, Ricard, & Villeneuve, 1997). These modern psychiatrists possessed a new perception of mental illness, one that saw it as an illness like any other and, importantly, could be cured. They. began to advocate for a more humane approach to psychiatry and actively sought to wrestle power away from the traditional psychiatrists and religious comm~nities and gain control of strategic posts in the mental health system (Dorvil, Guttman, Ricard, & Villeneuve, 1997).
Meanwhile, with psychiatric hospitals becoming understaffed and overcrowded, the quality of care and life for residents within them deteriorated dramatically. Several sometimes horrifying first-hand accounts of life within these hospitals from former patients began to reach the public, further shifting public opinion and pushing policy makers to initiate changes to the mental health system.
One particularly notable first-hand account was published in 1961 by Jean-Charles Pagé, a former resident of St-Jean-De-Dieu hospital in Montreal (now Louis-H-Lafontaine Hospital). His shocking book entitled «Les fous crient au secours» (Pagé, 1961) described the appalling living conditions and care provided to patients and shed more light on the exploitation of patient labourers.
Pagé's ~xperience initiated vigorous public debates about the deplorable state of affairs in Ouebec psychiatric hospitals, debates which served to mobilize various stakeholders, who pressured the government to adopt changes to its deficient system of care. The
government quickly responded and appointed three modern psychiatrists to examine the
problems and needs of Ouebec's psychiatric hospitals and formulate recommendations regarding the appropriate organization of services. A year later, the Bédard commission as it is known produced a report that would trigger the onset of the second major era of psychiatrie service organization in Ouebec, the era of deinstitutionalization and regionalization.
1.2.2. Work in the era of deinstitutionalization and regionalization
The Bédard commission played a pivotai raie in the reorganization of psychiatrie services in Ouebec in that it set the stage for a shift away from institutionalized care to community-based care, a process referred to as deinstitutionalization. The commission called for the creation of the Direction of psychiatric services within the Ministry of Health, an entity that would be responsible for carrying out the commission's recommendations for reform. Three main objectives guided this reform: 1) the provision of a greater accessibility to a wide range of psychiatric services in the community and the transfer of some patients from the psychiatric hospitals ta these community resources, 2) a greater follow-up of the patients that leave the hospitals, and 3) the creation of programs that would facilitate patients' rehabilitation and reinsertion into society (Dorvil, Guttman, Ricard,
&
Villeneuve, 1997).'Interestingly, the importance of work and employment was not lost on the members of the commission and the leaders of this reform. Indeed, the commission proposed measures that aimed ta support individuals' pursuit of work and professional integration. One such
proposition was the creation of sheltered workshops, defined as a place where patients could pursue productive and paid work in an understanding and non-competitive atmosphere (Ministère de la Santé et des Services Sociaux, 1962). According to the commission, the creation of these workshops, along with the establishment of half-way houses, would allow hundreds of people who did not need to spend their lives in the hospital to leave and live semi-independently in the community. The commission notes that they were inspired by England's pioneering rehabilitation services, where 90 such workshops employing roughly 100 people each had been established (Ministère de la Santé et des Services Sociaux, 1962).
ln addition, the Bédard commission also recommended that Quebec's Provincial Placement Office reorganize its specialized services and pay special attention to the rehabilitation of people with mental i"ness through work, as it had had success doing in the case of the physica"y handicapped. Again, England served as an inspiration, as the British government's «Disabled Persons Act» required that industries have at least 3% of their employees be people with either physical or mental disabilities. According to the commission's report, this policy had resulted in the hiring of over 200 000 people with mental i"ness in the year 1950 alone (Ministère de la Santé et des Services Sociaux,
1962).
While the reform guided by the Bédard commission led to several concrete changes in the locus of psychiatrie care, most notably through the creation of psychiatrie departments in the province's general hospitals and the establishment of multidisciplinary external clinical
teams that could offer treatment in the community, other services that were supposed to complement these clinical services did not take shape as quiékly (Dorvil, Guttman, Ricard,
&
V1l1eneuve, 1997). Indeed, as hospitals continued to significantly reduce their patient populations, too little was done to ensure that the appropriate community resources and social reinsertion mechanisms, such as patient follow-ups and work integration measures, were put in place" to maintain and support these individuals (Charbonneau, 2002; Dorvil, Guttman, Ricard, & Villeneuve, 1997; Goldner, 2002). According to Boudreau, «Half-way houses and sheltered workshops are part of the plans, the projects, but rarely make the transition from paper to concrete reality» (Boudreau, 1984, p. 127, translated to English). Part of the problem was that very few funds were injected to support the development ofservices that promoted the full integration of people into their community. Instead, for
many years the services that did appear in the community consisted mainly of personnel
transfers from psychiatric hospitals to the regional psychiatric departments, external clinics and day centres, services that ultimately remained under the management and control of
the hospitals3 (Ministère de la Santé et des Services Sociaux, 1998). The situation gave
rise to a phenomenon some actors have called «transinstitutionalization», or the
reproduction of the grim conditions of psychiatric hospitals by other institutions in the community (Davis, 2006). Indeed, the development of services aiming to fully integrate people into society and into the workforce remained unimportant to the dominant actors of that time period.
Transinstitutionalization continued throughout the 1960s and 1970s, affecting vocational
as weil as clinical services. Several psychiatric hospitals relocated their sheltered
workshops to community settings, a move that 'was coherent with the growing notion of
«normalization» (Gagnon, Pilon, & Wallot, 1981), i.e. the idea that that a person's
rehabilitation from mental illness would progress best if it took place in a normal community environment. Some hospitals were more successful than others however in setting up a variety of services that could support an individual's desire for normal work.
For example, in the early 1970s Robert-Giffard Hospital in Quebec City (then Sai
nt-Michel-Archange Hospital) succeeded in establishing four work-related programs, namely workshops to help former psychiatrie patients develop their skills and initiate them to the
world of work, an adapted work centre where workers engaged in tasks such as carpentry,
cleaning, product assembly and kitchen work, and two workshops in the Quebec Hilton
hotel, including one that involved competitive4 placem~nts (Gagnon, Pilon, & Wallot,
1981). Essential to the development of these programs was 1) program coordinators' belief that people with mental illness were capable of assuming responsibility for their social and economic autonomy and 2) the desire of these coordinators to «prove to the population in general and to employers in particular that people with mental handicaps
3 The domination of the mental health budget by psychiatrie hospitals was no accident, but indeed the work of
interests groups determined to maintain power, prestige and their recognition as experts by society.
4 ln this sense, competitive means that employees with mental illness were paid the same wages as other
were able to meet the norms and requirements of a regular job in the private sector» (Gagnon, Pilon, & Wallot, 1981).
Unfortunately, such perspectives were not widely held at the time and frustration and criticisms regarding the lack and poor quality of work integration programs were voiced as early as 1970. While the philosophy of normalization would often be cited in ministerial documents, health authorities neglected to provide service providers with the operational tools needed to translate this philosophy into reality (Gagnon, Pilon,
& Wallot
, 1981). In consequence, the overwhelming majority of programs that existed were axed almost entirely on occupational activities that never allowed people attain a level of employability sufficient enough for them to integrate the regular workforce (Dorvil, Guttman, Ricard, & Villeneuve, 1997). Workers would only often have access to dull, repetitive jobs in non-stimulating environments, with no possibility of obtaining a diploma or being promoted (Boudreau, 1984; Dorvil, Guttman, Ricard, & Villeneuve, 1997). As a result, these workers could toil monotonously for years in the workshops, losing ail hope of meeting the requirements and standards of the labour market. In addition, economic changes, including a rise in unemployment, made employers less willing to contract out to the sheltered workshops, further reducing the work options available. These factors led some members in the mental health field to question whether shelter~d workshops were really an appropriate and effective way of developing employability and supporting people's rehabilitation.The Ministry of Health's little success in putting in place appropriate community-based services to support the integration and maintenance of people with mental illness into the community had a number of important consequences. First and foremost, it accentuated the burden that weighed on families who were increasingly responsible for the care of a loved one with mental illness (Dorvil, Guttman, Ricard, & Villeneuve, 1997). These families would often see their routines disrüpted, their activities limited and their finances stressed, and ail the while never have access to information and supports that could help alleviate their problems. Adding to the problem was the overall dearth of employment and housing·options for individuals with mental health problems, a situation that gave rise to a sharp increase in poverty and homelessness in this population (Dorvil, Guttman, Ricard, & Villeneuve, 1997). Difficulties with respect to social reinsertion and integration also led to
-the phenomenon known as -the «revolving door syndrome», defined as psychiatrie patients' incessant back and forth between the psychiatrie hospital and a community that
could. not meet their needs5 (Dorvil, Guttman, Ricard, & Villeneuve, 1997). In his
description of the plight of the mentally ill in the post-deinstitutionalization era,
Charbonneau paints a grim picture, «Using few services, discrete in their suffering,
anonymous and forgotten, these people will slowly amass obstacles that, while remaining
invisible, will become more and more severe and indelible. Cited in government policies
but forgotten by programs and services, incapable of getting access to effective treatment and rehabilitation services, they'lI make several desperate attempts to integrate or
reintegrate the workforce and to insert themselves socially... However, their mitigated
success and repeated failure will finally wear on them ... Over the course of months and
years, these people would share their exclusion with a confusing diagnosis, a few
renewable prescriptions and a welfare cheque that condemns them to poverty. The
stagnation and weight of their sUffering would cause their partner, their friends and their
family to disappear. Their catastrophe will distance them from their children and atlack
their raison d'être ... These people will thus be forgotten, because we don't lock them up
anymore. They will become invisibre» (Charbonneau, 2002).
1.2.3. The emergence of alternative psychiatrie resources and community-grown
vocational services
Though work and employment programs increasingly fell outside the scope of the mental health system's priorities, they were still a major priority to families and especially people
with mental illness. In fact, these supports, so inaccessible to so many, have often been
the ones deemed most important by people with mental illness (Trainor, Pomeroy, & Pape,
1993).
Faced with a limited scope of services and an escalation in social problems, and buoyed
by the growing human and patient rights movements, a new movement of protest against
the psychiatrie establishment began to emerg~ and take hold over the course of the 1970s
5 To get a sense of the magnitude of the problem, in 1970, more than 70% of ail admissions to Louis-H Lafontaine hospital were actually readmissions of people previously admitted (Dorvil, 1987).
13
(Dorvil, Guttman, Ricard, & Villeneuve, 1997). The consequence was the emergence of various alternative psychiatric resources devoted to social reinsertion, housing, treatment, self-help, and defence of rights (Dorvil, Guttman, Ricard, & Villeneuve, 1997; Fleury & Grenier, 2004), services that were most often developed by families or individuals touched by mental illness (Davis, 2006).
The services offered by these groups in the community were based on a vision of mental illness that stood in stark contrast to the one that dominated in the medical and psychiatric community. For instance, the arrivai of psychotropic medications in the 1950s and other
advances in psychiatrie research6 contributed to the widespread adoption of a biomedical
focus by the mental health field, a view that would lead many health providers to place a greater emphasis on medical treatment than other aspects of care. As time passed however, it was becoming increasingly clear that these medications were not a panacea, causing many practitioners to be guarded in their prognoses, not wanted to incite false hopes in their patients (Davis, 2006). Indeed, sorne health providers, having witnessed patients' repeated setbacks and readmissions to the hospital, would lose hope altogether and feel powerless and pessimistic about individuals' chances of recovery (Charbonneau, 2002). Even worse, some of these attitudes would influence the perspectives of other actors outside of the health system, infiltrating the sectors of employment and education among others (Charbonneau, 2002).
Community groups, on the other hand, adopted very different perspectives of how to meet the wants and needs of people with mental illness. ' White and Mercier describe the approach adopted by these alternative, community-based groups in Quebec, «Alternative practices in the field of health distinguished themselves from institutionalized m·edical practices by emphasizing a holistic rather than biomedical approach, faith in a relationship of support between caregiver and client rather than one based on domination, a minimal amount of intervention rather than resorting to invasive technologies, and, above-all, the respect of the dignity, autonomy and abilities of the person» (White & Mercier, 1989). Rousseau echoes these assertions and emphasizes these resources' desire to take into
account an individual's «social, economic, cultural and affective environment» (Rousseau,
1993). This adoption a more holistic approach was undoubtedly influenced by the growing research on the determinants of health, which stressed that the health system represents only one of the many determinants of health and weil being (R. G . . Evans, Barer, & Marmor, 1994). Other authors have emphasized these groups' focus on· empowering people with mental illness and their desire to help people increase their autonomy and ability to assume responsibility for their rehabilitation and recovery (Charbonneau, 2002). Authors such as Lecomte have also made reference to these groups' belief that social networks offer therapeutic benefits to people with mental illness, «Humans are biological and psychological beings enmeshed in social networks... This social network is determinant to the extent that it facilita.tes, supports, or inhibits the bio-psychological development over the different stages of a human being's life ... It is particularly important when this being is faced with a difficulty, a crisis, or a ruptured relationship. The network must then mobilize and provide the help needed to establish a new psychological and social equilibrium. These relationships of support and help from the social network constitute the basis of the community support system with respect to the biological and psychological human» (Lecomte, 1986). Finally, the majority of these groups would value the principle of «people first» (Anthony, 1993) and share the belief that the way people interact with each other is more important than where these interactions take place. They denounced the depersonalization that people with mental illness increasingly experienced during their encounters with health providers. The spirit of the principle of «people first» is captured weil by Deegan, «Those of us who have been labelled with mental illness are first and foremost human beings. We are more than the sum of the electro-chemical activity of our brain .... We are people. We are people who have experienced great distress and who face the challenge of recovery» (Deegan, 1995).
This opposing conception of mental illness and how it should be treated is reflected in the types of rehabilitation and work integration services that these alternative psychiatric resources would develop over the next few decades. One example of a particularly successful model of services is the clubhouse mode/. The very first clubhouse was founded in the 1940s in New York, where a group of individuals who had recently been discharged from the same psychiatric hospital formed a mutual aid organization called WANA (We Are Not Alone) (Davis, 2006). This organization, which later became known
as Fountain House, aimed to be a restorative environment where people with mental
illness could go, receive support, and be surrounded by people who believed that their
recovery from mental illness was possible (International Center for Clubhouse
Oevelopment, 2008a). It has served as the model for ail other clubhouses around the
world, including the ones that would be developed in Canada. The International Center for
Clubhouse Oevelopment (ICCO) defines these clubhouses in the following way, «A
Clubhouse is first and foremost a community of people. Much more than simply a program,
or a social service, a Clubhouse is most importantly a community of people who are
working together toward a common goaL .. A Clubhouse is a membership organization,
and therefore the people who come and participate are its members. Membership in a
Clubhouse is open to anyone who has a history of mental illness. This idea of membership
is fundamental to the Clubhouse concept, as having membership in an organization
means that an individual has both shared ownership and shared responsibility for the
success of that organization. To have membership in an organization means to belong, to
fit in somewhere, and to have a place where you are always welcome ... Clubhouse
communities are built upon the belief that every member can sufficiently recover from the
effects of mental illness to lead a personally satisfying life. Clubhouses are communities of
people who are dedicated to one another's success -- no matter how long it takes or how
difficult it is. The Clubhouse concept is organized around a belief in the potential for
productive contributions from everyone, even the member struggling with the most severe
effects of mental illness» (International Center for Clubhouse Oevelopment, 2008b).
Among the fundamental elements of the clubhouse model is the «work-ordered day» and
its employment programs, most notably its transitional employment programs7. The
work-ordered day is an eight-hour period, typically Monday through Friday, where members work side by side with staff to accomplish the tasks needed ta keep the clubhouse
functioning. The work is organized into work units, these units representing members' first
opportunity to ease into the world of work and social interaction (Fountain House, 2008).
Traditional examples of work units are kitchen/care, janitorial/housekeeping, clerical work
(accounting work, preparing newsletters, etc.), security, social activity organization, etc.
7 Some clubhouses don't include transitional employment in their mix of services, whereas others have added
(Fountain House, 2008; Marrone, 1993). Clubhouse staffing levels, purposely kept low, promote productive co~tributions by members to the clubhouse and foster relationships that form the key ingredient in clubhouse rehabilitation (Fountain House, 2008).
ln addition to these work units are employment programs that offer members the chance to pursue paid employment outside of the clubhouse. In transitional employment (TE), members are offered the chance to develop their work skills in a part-time job for a limited time period, usually six to nine months (International Center for Clubhouse Development, 2008a). These transitional employment placements will represent for many clubhouse
members a first successful work experience outside of the clubhouse. Members are paid
at least minimum wage and are offered both on- and off-site support and encouragement from the clubhouse staff. On the other hand, one criticism of the TE approach has been that it tends to favour placements into entry-Ievel jobs, where it is easier and quicker to train employees, rather than more highly skilled «white collar» jobs (Marrone, 1993). TE thus seems much beUer adapted to the needs· of members who possess IiUle work experience or who have been out of work for several years, as opposed to those who have the skills and desire to rapidly integrate the regular workforce. Indeed, the program reflects the view that some members, because of skill deficits or lack of work experience, will always have difficulty securing employment (Marrone, 1993). Individuals who wish to obtain a regular job can be directed to what is sometimes called the independent employment program, where members can apply for work on their own and receive support from the clubhouse. However, members are generally encouraged to start in the TE program and use it as a potential stepping-stone to a competitive job (Fountain House, 2008).
Another well-known organization that provided a model of vocational services' is Thresholds, one of the oldest psychiatrie rehabilitation centres in the United-States8.
Guided by the principle that «Everyone contributes to society ... Everyone has untapped potential, with gifts and skills to develop» (Thresholds, 2008), Thresholds would see its
8 Thresholds was founded by the National Council of Jewish Women, after several members had attended a conference on mental health. Sympathetic to the plight of people with mental illness, they established this rehabilitation agency in the face of discouragement from most mental health experts they had consulted.
vocational services expand over the course of the 1970s and 1980s. Like in the clubhouse model, new members would be encouraged to join a work crew (similar to the Clubhouse concept of work units) that would allow them to practice various kinds of job skills (Cook & Razzano, 1992). When ready, members could take advantage of a paid group placement or a more independent form of employment. This latter service would initially consist of a transitional employment program but would eventually be altered to provide more flexible placements that no longer needed to be temporary (Cook & Razzano, 1992). Responding to the expressed needs of their members, the agency would also develop two other innovative services, namely the creation of member-run businesses (for example, delivery services, catering services, printing/copying services) and mobile job support team made up of staff members who could provide regular ongoing vocational support or intervention at the work site (Bond, Drake, Becker, & Mueser, 1999; Cook & Razzano, 1992).
These ideas and models of work integration services, often originating in the United-States or abroad, would slowly disseminate and inspire community groups in Canada. Beginning in the late 1970s and continuing into the turn of the century, an increasingly broad range of alternative resources and community services would emerge. The growth of these community groups would at times be stunted, however, by various factors including a lack of funding and a lack of recognition from health authorities and the medical establishment ,. (Dorvil, Guttman, Ricard, & Villeneuve, 1997). Nevertheless, in Ouebec, determined organizations devoted to developing employability, professional training, work integration through internships, management of social enterprises and integration to competitive employment would eventually emerge ail over the province, with the majority of services congregating in larger urban centres like Montreal, Laval and Ouebec City (Charbonneau, 2002; Latimer & Lecomte, 2002).
These new programs would come to co-exist with the vocational services that were being developed and managed in parallel by the psychiatric community. In the early 1980s in Ouebec, the network of sheltered workshops, which had become increasingly criticized and viewed as insatisfactory, was split into two separate networks, a network of skills
development programs offered by rehabilitation centres9 and a separately-funded network of adapted work centres 10 (Dorvil, Guttman, Ricard, & Villeneuve, 1997). The same time period would also see the creation of new programs and measures by the Ministry of Employment that aimed to increase the social and economic contribution of people with handicaps. For instance, the early 1980s saw the creation of subsidies offered to employers to compensate them for the potentially increased costs of hiring a person with a handicap 11, as weil as various other forms of financial incentives for unemployed individuals and welfare recipients. Furthermore, in the mid-1980s, various community organizations interested in the social and professional insertion of various clienteles were regrouped together under the program service externe de main d'oeuvre (SEMO), thus adapting their missions to focus on the integration of people with handicaps into the regular workforce. Indeed, over the years new stakeholders from a variety of sectors would join the cause, giving rise to a diversity of vocational approaches and giving birth to new concerns with regards to the continuity and efficiency of services.
While a greater variety of vocational supports and services were gradually coming to light, some actors maintained that many of these approaches still suffered from a variety of weaknesses. Among the criticisms were that: 1) programs often encouraged or required individuals to engage in unpaid prevocational services, even after these individuals had expressed interest in being placed rapidly in 'competitive employment; 2) individuals participating in work units or work crews would often stay in these types of jobs for extended periods of time, rarely progressing to competitive employment; 3) protected work environments, where the majority of employees have disabilities, are less normalizing than regular work environments and prevent people with mental illness from having contact with nondisabled workers; 4) in traditional rehabilitation programs, the starting point for locating
9 Les services d'apprentissage aux habitudes de travail (SAHT) were in essence still sheltered workshops.
10 Adapted work centres (CT A) are defined as organizations that offer long-term employment possibilities to people with physical and mental handicaps who are seen as having major limitations that prevent them fram integrating the regular workforce (L'Office des personnes handicapées du Québec, 1997). CTAs 'must employ, at ail times, a number of individuals with disabilities that represents at least 60% of its total number of employees.
jobs is determined largely by these programs' relationships with employers and not by the preferences .of clients (Bond, Drake, Becker, & Mueser, 1999). Faced with these perceived weaknesses, some of these actors would advocate for a different approach to vocational services, one that would emphasize the importance of competitive employment in integrated work settings and with follow-along social and professional supports.
1.3. Supporled employment
An extensive literature exists on the topic of supported employment, dating back ta its early beginnings as a program designed to assist individuals with developmental disabilities. In the following chapters, 1 will briefly discuss the origins of this model of
services, describe its key principles and provide an overview of efforts to implement this model in a Canadian context.
1.3.1. Origins and principles of the supported employment model
The origins of the supported employment model can be traced back to the late 1970s and a supported competitive employment program at Virginia Commonwealth University's Rehabilitation and Training Centre. This program, founded by Dr. Paul Wehman and his associates, was conceived as a means for people with severe developmental disabilities to integrate competitive work settings and work side-by-side with non-disabled persons (Wehman & Moon, 1988). Indeed, the fundamental assumption of supported employment is that ail person's, regardless of extent or nature of disability, should have an opportunity to work in the community (Wehman & Moon, 1988). In this spirit, the program developed in Virginia sought to place people rapidly in competitive employm~nt and provide the intensive support needed to help them maintain their job.
The program would prove to be an effective way of helping peopl~ with disabilities integrate the regular workforce. News of the program's success would disseminate and arouse great interest in the vocational rehabilitation field. In particular, some stakeholders believed that such programs could also be effective for other populations, including people with severe mental illness (Mellen & Danley, 1987). Early experiments with this clientele took place in New Hampshire in the early 1990s as community mental health centres looked to implement supported employment programs and transition away from day
centres. Though the transition away from day centres, perceived to be a safety net for people with mental illness, provoked fear and concern from service users, families and clinicians, vocational outcomes proved to be more positive than expected, facilitating the programs' acceptance (Drake, 1998).
While Wehman's program for people with disabilities clearly influenced the vision underpinning the programs developed for a mental health clientele, it was not the only source of influence. Indeed, aspects of these programs were also influenced by the development of Assertive Community Treatment (ACT) and by the professional and clinical experiences of the program founders (Bond, 1998). These latter individuals would in essence take the best ideas from the literature, adapt them for a clientele with mental illness and standardize them so that a minimal level of quality could be achieved in different contexts (Bond, 1998). This process has produced resulted in a model of supported employment that is characterized by several guiding principles (Bond, 2004):
Competitive employment is the goal Eligibility is based on consumer choice Rapid job search
Integration of vocational rehabilitation and mental health • Attention to consumer preferences
Individualized and time-unlimited support
The first principle guiding supported employment programs is that the goal for clients is competitive employment in integrated work settings, i.e. where the majority of employees do not have disabilities. This principle is based on the belief that most people with severe mental illness can achieve competitive employment (Bond, 1998). It is argued that integrating clients into work settings where they are surrounded by colleagues without disabilities fosters a greater sense of normalcy and facilitates a more complete integration into the community, as clients are encouraged to move out of patient roles and adopt normal adult roles (G. R. Bond, Salyers, Rollins, Rapp, & Zipple, 2004).
The second principle of the supported employment model relates to programs'
inclusion/exclusion criteria. Essentially, programs are available to any person with a mental illness who expresses the desire to work in a competitive environment. Like in the supported employment program founded by Wehman, the nature and extent of the illness or disability is not an exclusion criteria. Furthermore, individuals are not excluded on the basis of their «work readiness» or perceived capacity to work (G. R. Bond, 2004).
Rapid job search is the third principle that guides these programs. This principle distinguishes them from other vocational services that aim for competitive employment in that efforts are not made to provide clients with extensive prevocational skills training or pre-employment assessments. Instead, the goal is to move the individual directly into a meaningful job and surround that person with the supports (for example, work accommodations, on-the-job training, psychosocial or socio-professional support) necessary to maintain that job. It is
a
«place-train» rather than a «train-place» philosophy (Drake, 1998). According to the founders of the model, there is little empirical evidence to support the view that approaches that favour lengthy pre-employment assessment,training and counselling help people obtain jobs or keep them longer (Bond, 1998).
Indeed, some evidence suggests that such approaches actually reduce people's chances of achieving competitive employment (Bond, 1992).
The fourth principle, the close integration of vocational rehabilitation and clinical treatment teams, is a cardinal feature of the model and one that was inspired by the ACT model (G. R. Bond, 1998). The rationale underlying the historical non-integration of services was that rehabilitation services should be provided exclusively by specialists in rehabilitation and that clinical environments were typically stigmatizing and dominated by medical perspectives (Drake, Becker, Bond, & Mueser, 2003). However, integration at a client-level, such as the development of multidisciplinary teams, tend to promote services that are better tailored to the individual client and have been shown to lead to better clinical and vocational outcomes (Cook, Lehman et aL, 2005; Drake, Becker, Bond, & Mueser,
2003). According to the model's founders, the best way to achieve this integration is to have the vocational rehabilitation staff work at the same agency and even be part of the same team as the clinical treatment staff. They argue that while many attempts to
integrate these two fields have been made, whether it be through interagency agreements, cross-training or other strategies, the fact that there are multiple providers involved makes communication and service coordination difficult and poses a challenge to clients who must negotiate with numerous agencies (Bond, 1998). Drake describes four benefits to achieving· integrated vocational and clinical services: 1) more effective engagement and retention of clients, 2) betler communication between employment specialists ,and mental heâlth clinici'ans, 3) clinicians learn to appreciate the value of work and as such focus more on it when meeting with patients, and 4) the incorporation of clinical information into vocational plans (Drake, Becker, Bond, & Mueser, 2003).
The emphasis placed on client preferences, the fifth principle, is consistent with the trend of client-centred service, delivery and care and supported by evidence on vocational outcomes and work satisfaction. For example, when a job placement matches an individual's work preferences, they tend to be more satisfied with the job and likely to remain in it (Bond, 2004). According to the founders of the supported employment model, many other vocational programs ignored client preferences because they only offered clients the jobs that were made available by pre-established relationships with employers. Furthermore, Bond remarks «If consumer preferences were the deciding factor in the design of vocational programs, it is questionable that unpaid work units would be such a prominent feature in so many agencies. The reality is that providers usually make choices for consumers about the structure and pacing of vocational services, regardless of what consumers say they want» (Bond, 1998).
The last principle, time-unlimited and individualized support, is a fundamental tenet of the mode!. Inspired again by Wehman's vocational program, it is understood that vocational success is directly related to the duration and individualized nature of support that is offered to clients. In other words, it has to be there when they need it and must accommodate their unique needs. The time-unlimited nature of support is also viewed as central given the episodic nature of many mental illnesses. Also, cQnsistent with the view that rehabilitation services should promote the autonomy of people with mental illness, such support can be tapered-off gradually as the individual's independence increases.
23
It is important to note that as time has passed, several other principles have been .
considered as being important elements of supported employment. For instance, some authors have emphasized the importance of counselling clients on the impact that competitive employment could have on their disability benefits (Tremblay, Smith, Xie, &
Drake, 2006). Others have highlighted the need for creating of a therapeutic alliance between the client and employment specialist (Catty et aL, 2008), negotiating work accommodations (MacDonald-Wilson, Rogers, Massaro, Lyass, & Crean, 2002), involving family members and developing career plans (Corbière, Submitted). Still others have emphasized making good job matches and adopting a recovery approach (G. R. Bond, 2004). As mentioned by Bond, «additions, refinements and deletions are ail ongoing processes in an empirical approach to defining an evidence-based practice» (Bond, 2004).
While these other principles may be regarded as important elements of supported employment, they have generally been less studied than the· original six principles which remain the most commonly identified principles ~f the supported employment model. Programs that adhere closely to these six key principles can be said to follow the Individual Placement and Support (IPS) model of supported employment, described as the standardized version of supported employment specifically for people with severe mental illness (Bond, 2004). IPS programs are further characterized by a variety of critical program components, such as small caseload sizes (ideally less than 25 clients per employment specialist), vocational' generalists (each employment specialist carries out ail phases of the vocational service), vocational units (employment specialists form a vocational unit with group supervision), and community-based services (employment specialists spend at least 60% of their time in the community and outside of their offices) (Bond, Becker, Drake, & Vogler, 1997). IPS is thus typically distinguished from other forms of supported employment that may adhere less closely to the six guiding principles and other components of the supported employment model or may cater to clienteles not having a severe mental illness (Dartmouth Supported Employment Center)12.
12 For an exhaustive list