Low-value hospitalisations following injury: a
multicenter cohort study
Mémoire
Marc-Aurèle Gagnon
Maîtrise en épidémiologie - avec mémoire
Maître ès sciences (M. Sc.)
Résumé
Les soins de faible valeur entraînent des coûts considérables et exposent les patients à des événements indésirables. On estime que les soins de faible valeur pourraient représenter jusqu’à 30% des coûts des systèmes de santé, mais peu d’information existe sur les hospitalisations de faible valeur chez les victimes de traumatismes. Nous avons réalisé une étude de cohorte rétrospective multicentrique sur tous les patients admis dans un centre de traumatologie désigné au Québec sur 5 ans afin de combler un manque de connaissances sur le sujet. La prévalence d’hospitalisations de faible valeur dans le système de traumatologie du Québec était de 16% et nous avons identifié des groupes au sein desquels cette prévalence était plus élevée. Nous avons également observé une forte variation inter-hospitalière dans cette prévalence. Nos résultats suggèrent qu’il s’agit d’un problème important, qu’une amélioration de la situation est possible, et indiquent des groupes prioritaires à cibler.
Abstract
Evidence of low-value care around the world is growing, representing increased costs and worse outcomes for patients. Low-value care has been estimated to represent up to 30% of hospital resources, but little information is available on low-value hospitalisations following injury. We conducted a multicenter retrospective cohort study on all patients admitted to any trauma center in the province of Quebec between 2013 and 2019 to fill a knowledge gap on these hospitalisations. We observed a prevalence of low-value hospitalisations of 16%, identified patient groups with a high prevalence, and observed strong inter-hospital variation. Our results demonstrate that low-value hospitalisations following injury are an important problem, that there is a potential for improvement, and they identify patient groups which could be good targets for interventions seeking to reduce low-value care in this population.
Table of contents
Résumé ... ii
Abstract ...iii
Table of contents ... iv
List of tables ... vi
List of figures ... vii
List of acronyms ... viii
Acknowledgements ... ix
Foreword ...x
Introduction ... 1
Chapter I. Literature review ... 2
1.1 – Burden of injuries in Canada ... 2
1.2 – Low-value care ... 2
1.3 – Low-value hospitalisations ... 3
1.4 – Low-value care in injury ... 3
1.5 – Low-value hospitalisations in injury ... 4
Chapter II. Objectives ... 6
Chapter III. Methods ... 7
3.1 – Study setting and population ... 7
3.2 – Study data ... 8
3.3 – Identifying low-value hospitalisations ... 8
3.4 – Assessing inter-hospital variation ... 9
3.5 – Treatment of missing data ... 10
Chapter IV. Low-value hospitalisations following injury: a multicenter cohort study ... 11
Résumé ... 12
Abstract ... 13
Introduction ... 14
Methods ... 14
Study Design & Population ... 14
Study Data ... 15
Selection of Criteria to Identify Low-Value Hospital Admissions ... 15
Sensitivity analyses ... 16
Results ... 17
Sensitivity analyses ... 18
Discussion ... 19
Strengths and limitations ... 21
Impact and future research ... 22
Conclusion ... 23
Chapter V. Discussion ... 36
5.1 – Summary of results in line with objectives ... 36
5.2 – Comparison with the literature ... 36
5.3 – Internal validity ... 37 5.3.1 – Selection bias ... 37 5.3.2 – Information bias ... 38 5.3.3 – Confusion bias ... 38 5.4 – External validity ... 39 6.0 – Conclusion ... 39 References ... 40
List of tables
Table 1. Advisory committee ... 9
Table 2. Description of the study population ... 25
Table 3. Imagery use by age group in potentially low-value hospitalisations ... 29
Table 4. Length of stay and cost estimation in potentially low-value hospitalisations ... 30
Table 5. Sub-group analysis: inter-hospital variation by age group ... 33
List of figures
Figure 1. Algorithm to select potentially low-value hospitalisations ... 24 Figure 2. Most frequent primary diagnoses by age group ... 27 Figure 3. Therapeutic interventions by age group and diagnosis among potentially low-value hospitalisations ... 28 Figure 4. Adjusted prevalence of potentially low-value hospitalisations by hospital and trauma center designation level ... 32
List of acronyms
ED Emergency department
FAST Focused assessment with sonography in trauma
CT Computed tomography
TBI Traumatic brain injury GCS Glasgow coma scale score ICC Intraclass correlation coefficient AIS Abbreviated injury scale
Acknowledgements
I would like to express my most sincere gratitude and appreciation to my supervisor Dr. Lynne Moore. Through her dedication to helping her students progress and learn, she has been a more supportive and helpful supervisor than I ever would have dared hope for. I would also like to thank my co-supervisor Dr. Mélanie Bérubé for her general help and her clinical expertise which has been invaluable for this project.
Finally, I would like to thank everyone with whom I have had the pleasure of working throughout my project: Amina, Kahina, Pier-Alexandre, Xavier, Abakar, Blanchard, Thowiba, Samie and Khadidja for their help and support, and for creating an amazing work environment.
Foreword
This thesis was written as part of my master’s degree in epidemiology under the supervision of Dr Lynne Moore. The fourth chapter of the thesis consists of the article “Low-value hospitalisations following injury: a multicenter cohort study” which will be submitted to the Canadian Medical Association Journal. I am the first author of the article, and was responsible for the literature review, the analyses, and writing the article. The coauthors of the article are Mélanie Bérubé, Amina Belcaid, Alexis Turgeon, François Lauzier, Gilles Bourgeois, and Lynne Moore.
A protocol of this project was presented at the following events:
1. Journées de la recherche du CHU de Québec-Université Laval in May 2019 2. Journée de la recherche des étudiants de l’axe SP-POS in June 2019
The results of the article were presented at the following events:
1. Oral presentation at the Soirée de la recherche de la division de soins intensifs du
département d’anesthésiologie et de soins intensifs in November 2019
2. Oral presentation at the Colloque trauma Défis! 2020 du CHU de
Québec-Université Laval in February 2020
3. Oral presentation to the INESSS (Institut national d’excellence en santé et services
sociaux) in February 2020.
The abstract was also chosen for presentations at the following events:
1. Oral presentation at the Trauma Association of Canada Annual Meeting & Conference in March 2020 (conference cancelled due to COVID-19 outbreak) 2. Oral presentation at the Choosing Wisely Canada National Meeting in May 2020
(presentation cancelled due to COVID-19 outbreak)
3. Poster presentation at the IXe Congrès International d’Épidémiologie
I received a travel bursary for my presentation at the Journée de la recherché des étudiants
de l’axe SP-POS and was awarded a prize for best presentation at the Colloque trauma Défis! 2020.
Introduction
Injury is a considerable burden for society, representing around 16,000 deaths, 60,000 disabilities, 3.5 million visits to emergency departments (ED), and 27 billion dollars each year in Canada1. There are over 230,000 hospitalisations for injury care each year in Canada with an average length of stay of over 9 days, and a conservative estimated cost of $10,971 per hospitalisation1, 2.
Evidence suggests that around 30% of healthcare budgets are spent on low-value care, which can be defined as the provision of medical services for which the potential for harm
exceeds the potential for benefit3-5. If these figures apply to hospitalisations, then it is likely
many patients are hospitalized without need. In addition to wasting resources, low-value hospitalisations expose patients to hospital-related adverse events such as nosocomial infections, functional decline, psychological distress and potential loss of revenue6. Therefore, a reduction in low-value hospitalisations has the potential to yield major benefits by both allowing resources to be reallocated towards appropriate care and improving patient outcomes.
Most of the literature on avoidable hospitalisations focuses on the prevention of certain conditions requiring hospitalisation rather than on the prevention of hospitalisations per se 7-9
. A recent scoping review identified specific circumstances in which injury hospitalisations could be low-value10. For example, adults with blunt abdominal trauma with a normal physical exam and a negative FAST (focused assessment with sonography in trauma) or CT (computed tomography) or adults with mild traumatic brain injury, a normal CT scan and a normal clinical exam who are not on anticoagulation therapy10. However, these identified practices probably represent a fraction of low-value hospitalisations in injury care and there is a knowledge gap on their prevalence. A study with a broader scope could both provide the estimates of prevalence which are missing from previous studies and a new perspective from which to identify low-value hospitalisations, therefore filling a major knowledge gap.
Chapter I. Literature review
1.1 – Burden of injuries in Canada
Each year in Canada, injuries cause around 16,000 deaths and over 60,000 disabilities, and the number of deaths are expected to rise to over 26,000 by 20351. In the age group of 1 to 44, preventable injuries are the first cause of death for Canadians and they lead to over 500,000 potential years of life lost every year1. Injuries also cause 3.5 million visits to the ED and over 230,000 hospitalisations in Canada annually1. Injury therefore represents a considerable burden to society, not only in terms of years of life lost, but also in resources for healthcare providers. The total economic costs of injury in Canada per year is around 26.8 billion dollars; 15.9 billion in direct health care costs and 10.9 billion in indirect costs due to loss of productivity, and this number is expected to increase to $75 billion by 20351. A conservative estimate for the costs of hospitalisations in injury care alone reaches over $2.5 billion2.
1.2 – Low-value care
The Institute of Medicine defines low-value care as the provision of medical services for
which the potential for harm exceeds the potential for benefit3, 5. A study in the United States estimated low-value care to represent up to 30% of all health care spending4, 11. Drivers of overuse include financial incentives, the fear of missing diagnoses, medico-legal concerns, and lack of strong evidence base for clinical practices12. Fee-for-service payment systems encourage care providers to offer as many services as possible to maximize their financial gains12. Clinicians may go against guidelines and prescribe too many tests by fear of either compromising the patient’s safety or a potential lawsuit. Poorly informed patients may push for certain interventions because of a marketing campaign or anecdotal evidence12. Indication creep is also a common way in which low-value care develops; a new treatment gains interest and is offered to more and more patients until it is offered to patients in whom its benefits are not supported by evidence13.
In a recent Canadian study, low-value procedures were associated with an incidence of hospital-acquired complications of up to 15%14. These complications also on average
doubled the median length of stay of patients, further exposing them to hospital-related adverse events14. Older adults are particularly impacted by this increased length of stay due to their vulnerability to functional decline and pressure ulcers caused by low mobility15. Children are vulnerable to significant increases in lifelong risks of cancer associated with the unnecessary imaging that often follows low-value hospitalisations16, 17. All patients are vulnerable to increased risks of nosocomial infections. The Choosing Wisely campaign collaborates with groups of physician to produce evidence-based guidelines and recommendations on practices that should be avoided in order to reduce low-value care13.
1.3 – Low-value hospitalisations
The literature on preventable hospitalisations often revolves around ambulatory-care sensitive conditions7-9. These are defined as conditions which can be prevented or treated through outpatient care, for example conditions for which vaccines are available or management of complications of chronic diseases, such as diabetes18. These low-value hospitalisations can be caused by factors such as unavailability of primary care, delayed care given by physicians, delayed help sought by patients, or absence of social support for the patient9. In a study of ambulatory-care sensitive conditions in Germany, physicians considered 41% of the hospitalisations to have been potentially avoidable. A study of those eligible for Medicare or Medicaid in the United States found 26% of all hospitalisations to be potentially avoidable7. An initiative aiming to reduce avoidable hospitalizations for patients residing in nursing homes in Missouri attained a 30% reduction in all-cause hospitalization8. These results demonstrate that considerable gains could be made with improved prevention and primary care. However, there is a knowledge gap on the prevalence of low-value hospitalisations following traumatic injuries.
1.4 – Low-value care in injury
Previous studies have found significant variation in patient outcomes between trauma centers19. In addition, suboptimal care has been documented in up to 50% of hospitalisations19. These figures suggest the presence of low-value care for injury hospitalisations.
Choosing Wisely Canada has produced recommendations regarding practices which should
be questioned, a few of which concern trauma care. For example, head CT scans for patients presenting with minor head injury and whole-body CT scans for minor or localized trauma in both adult and paediatric populations.
A recent scoping review identified 63 practices that were identified by at least one empirical study as low-value and considered by at least 70% of experts consulted as clearly or potentially low-value. However, we lack data on the prevalence of these practices. This may be due to lack of detailed clinical data allowing identification of specific patient populations or clinical practices3.
1.5 – Low-value hospitalisations in injury
Of the 63 practices identified in the aforementioned scoping review, 6 of them relate to low-value hospitalisations:
Hospitalisation in adult blunt abdominal trauma with normal physical exam and negative FAST or CT.
Hospitalisation in paediatric blunt abdominal trauma with normal physical exam, asymptomatic and negative FAST or CT.
Hospitalisation in stable anterior abdominal stab wound, negative on FAST or CT and negative local wound exploration.
Hospitalisation in mild TBI (traumatic brain injury), negative on a validated clinical decision rule or normal CT and normal clinical exam, not on anticoagulation therapy.
Hospitalisation in pediatric isolated skull fracture with Glasgow Coma Scale score (GCS) =15, normal neurological exam and low-energy injury mechanism.
Hospitalisation in isolated sternal fractures with normal cardiac enzymes (troponin) and normal electrocardiogram.
However, these identified practices probably represent only a fraction of low-value hospitalisations in injury care and there is a knowledge gap on their prevalence.
The burden that hospitalisations following injury represent, both in costs and consequences for patients and evidence of the presence of low-value care suggest that interventions targeting reductions in low value injury hospitalisations have the potential to improve the quality and efficiency of acute injury care. However, before actions can be taken, more information is needed on the prevalence and characteristics of low-value hospitalisations to inform the development of high-impact interventions.
Chapter II. Objectives
The main objective of this study is to advance knowledge on low-value hospitalisations following injury. The specific objectives are as follows:
1. Estimate the prevalence of low-value hospitalisations following injury 2. Identify patient groups with a high prevalence of low-value hospitalisations 3. Assess inter-hospital variation in the prevalence of low-value hospitalisations
Chapter III. Methods
Methods are explained in the article presented in chapter 4. Chapter 3 will be used to give further details on specific aspects of methodology which could not be included in the article.
3.1 – Study setting and population
The Quebec trauma care continuum is a network of coordinated trauma centers which work together to provide personalized care to trauma victims. This coordination seeks to ensure that patients get the most appropriate care regardless of their geographical location or the severity of their injuries. There are 59 trauma centers separated into 4 different levels, and each level has a specific purpose in the system. The categories follow American College of Surgeons’ recommendations20, 21
:
Level I trauma centers (n=5, two of which are paediatric) are large urban hospitals, offering ultra-specialized care in neurotraumatology and orthopaedic surgery, and have advanced interdisciplinary rehabilitation services. They are located in the most populated cities and have the highest patient volume.
Level II trauma centers (n=5) offer similar services to level I centers but are situated in smaller cities and have lower volume.
Level III trauma centers (n=21) are located in less densely populated areas and provide expertise in general surgery, orthopaedic surgery and intensive care.
Level IV trauma centers (n=28) are mostly situated in remote areas and are equipped to treat trauma of moderate severity and to stabilize patients suffering from major trauma to allow for safe transfer to a more specialized center. They offer general surgery and anaesthetic services.
The population for this study is comprised of all patients admitted to any of the 59 trauma centers in the province of Québec following injury from April 1st, 2013, to March 31st, 2018. We excluded deaths on arrival and patients who left against medical advice.
3.2 – Study data
The Quebec Trauma Registry was introduced in 1998 with the purpose of providing data for the evaluation and improvement of the quality of provincial trauma care. Every trauma center in the province has the obligation to enter all ED deaths and hospitalisations with a primary diagnosis of injury in the registry. Data are centralized at the Ministry of Health. The registry contains information on around 75% of all injury hospitalisations in the province; other cases are admitted in non-designated hospitals22. The registry includes information on socio-demographics, circumstances of the injury, vital signs on arrival, transfer status, diagnostic codes, interventions, admission services, complications, comorbidities, dates and times of admission and discharge and discharge destination. Data is entered by medical coders who undergo standardized training to ensure uniformity23. Coders participate in discussion forums and thrice-yearly meetings with clinicians to discuss coding queries. The registry also contains built-in algorithms to avoid coding errors and following yearly aggregation, data managers check data to correct abnormalities23.
3.3 – Identifying low-value hospitalisations
To identify potentially low-value hospitalisations, we created an algorithm using criteria which aimed to single out patients who did not require hospitalisations. Criteria used were in-hospital death, injury severity, GCS, surgery or other interventions requiring hospitalisation, admission to critical care unit, transfer to an acute care center or referral for rehabilitation (Supplemental digital content 1). The algorithm was derived using criteria developed on consultation with a panel of experts (Table 1).
Table 1. Advisory committee
Committee member Expertise
Mélanie Bérubé Trauma advanced practice nurse / trauma care coordinator
Éric Mercier Emergency physician
Alexis Turgeon Critical care physician / anesthesiologist François Lauzier Critical care physician / internist
Jean Lapointe Emergency physician / trauma system manager
Gilles Bourgeois General practitioner / trauma system manager
Julien Clément Trauma director / trauma surgeon
Patrick Archambault Emergency physician / critical care physician Christine Rizzo Trauma nurse/ trauma care coordinator Amina Belcaid Trauma data expert
3.4 – Assessing inter-hospital variation
To assess inter-hospital variation, the association between our exposure (the trauma center) and our outcome (the provision or not of a potentially low-value hospitalisation) was measured while adjusting for patient level risk factors. Since our outcome was dichotomous and relatively common (>10%), we decided to use a robust Poisson model which also has the advantage of producing risk ratios and being less susceptible to model misspecification24. Trauma centers were modelled as random intercepts and patient level risk factors were modeled as fixed effects (age, sex, New Injury Severity Score, GCS, injury mechanism, number of injuries, primary injury diagnosis and number of comorbidities). Variables were tested for linearity and, in cases where the assumption was not met, we created categories based on well-documented cut points for each variable25, 26. The measure used to quantify the inter-hospital variation was the intraclass correlation coefficient (ICC), which reports the correlation between observations within the same
cluster. It can be interpreted as the amount of inter-hospital variation that is not accounted for by covariates. Cut points taken from the literature were used to classify the variation as weak (ICC=0-5%), moderate (5-20%) or strong (>20%)27.
3.5 – Treatment of missing data
One of the variables used in the model, the GCS, was missing for 50% of the patients. This issue was addressed using multiple imputation, a method in which a predictive model is used to generate multiple plausible values to replace missing values based on correlated variables. For this method to produce valid results, the data must be missing at random, which means that the probability of missing data on a variable can be predicted using other measured variables. We believe this assumption to be reasonable since factors such as the injury and its severity may predict the absence of GCS evaluation, which is often not evaluated in patients with a minor extracranial injury. Simulation studies have shown multiple imputation of the GCS to lead to valid effect estimates when the imputation model is correctly specified28. The imputation model included all dependant and independent variables used in the analysis models. We used 50 imputations, based on the percentage of patients with a missing GCS. We modelled the GCS as a series of indicator variables, representing each of its values (with 15 as the reference category), and retransformed to its original scale using adaptive cut points29.
Chapter IV. Low-value hospitalisations following injury: a multicenter
cohort study
Marc-Aurèle Gagnon, Msc Candidate1,2, Mélanie Bérubé, PhD2,3, Amina Belcaid, Msc4, Alexis Turgeon, MD, Msc1,2,5, François Lauzier, MD, Msc2,6, Gilles Bourgeois, MD7, Lynne Moore, PhD1,2
1
Département de médecine sociale et préventive, Université Laval, Québec, Qc, Canada 2
Axe Santé des Populations et Pratiques Optimales en Santé (Population Health and Optimal Health Practices Unit), Traumatologie – Urgence – Soins intensifs (Trauma – Emergency – Critical Care Medicine), Centre de Recherche CHU de Québec – (Hôpital de l'Enfant-Jésus), Université Laval, Québec, Qc, Canada
3
Faculté des sciences infirmières, Université Laval, Québec, Qc, Canada 4
Institut National d'Excellence en Santé et Services Sociaux, Montréal, Qc, Canada 5
Département d’anesthésiologie et de soins intensifs, Université Laval, Québec, Qc, Canada 6
Département de médecine interne, Université Laval, Québec, Qc, Canada 7
Urgences-Santé, Montréal, Québec, Canada
Corresponding author and address for reprints:
Marc-Aurèle Gagnon
CHU de Québec – Université Laval Research Center (Hôpital de l’Enfant-Jésus) Population Health and Optimal Health Practices Research Unit, Trauma – Emergency – Critical Care Medicine
1401, 18ème rue, local Z-201, Québec (Qc), G1J 1Z4, Canada Phone: 418-649-0252 ext. 3366
Fax:
Email: [email protected]
Disclosure:
This research was supported by the Canadian Institutes of Health Research (Foundation grant, #353374 and Embedded Clinician Researcher (PA)). Drs Moore, Lauzier, and Bérubé are recipients of a research salary Award from the Fonds de Recherche du Québec – Santé (FRQS). Dr Turgeon is the Canada Research Chair in Critical Care Neurology and Trauma.
Résumé
Contexte : Au Canada, les blessures engendrent chaque année 260,000 hospitalisations et 27 milliards de dollars en coûts. Des études indiquent qu’environ 30% de ces dépenses pourraient être superflues. En plus des pressions exercées sur le système de santé, les hospitalisations de faible valeur comportent des risques importants pour les patients (événements indésirables, déclin fonctionnel).
Objectifs : Calculer la prévalence d’hospitalisations de faible valeur à la suite de blessures, déterminer les groupes de patients chez qui cette prévalence est élevée et en mesurer la variation inter-hospitalière.
Méthodes : Après une revue de la littérature scientifique et une consultation auprès d’experts, nous avons élaboré un algorithme pour isoler les hospitalisations potentiellement de faible valeur d’avril 2013 à mars 2018 dans un système de traumatologie canadien inclusif. Après avoir déterminé les groupes à fréquence élevée, nous avons utilisé un modèle de régression de Poisson robuste multiniveaux pour estimer la variation inter-hospitalière, à l’aide de coefficients de corrélation intraclasse (ICC). Les analyses ont été stratifiées par âge (1-15; 16-64; 65-74; 75+).
Résultats : La prévalence des hospitalisations à faible valeur s’élève à 16% (19,155/118,032) tous groupes confondus, à 26% (2,126) en pédiatrie, à 11% (4,693) chez les jeunes adultes et à 19% (12,336) chez les aînés. Les diagnostics les plus fréquents étaient : traumatisme crânien cérébral léger chez les enfants (43% des occurrences chez les patients pédiatriques; n=922); blessure superficielle (14%; n=660), blessure mineure à la colonne (14%; n=634) et traumatisme crânien cérébral léger (11%; n=534) chez les jeunes adultes; et blessure superficielle chez les aînés (22%; n=2,771). Nous avons observé une forte variation inter-hospitalière dans la prévalence des hospitalisations de faible valeur (ICC=37%).
Conclusion : Une hospitalisation pour blessure sur six est potentiellement de faible valeur. Les groupes diagnostiques susmentionnés pourraient faire l’objet d’études futures visant à réduire la surutilisation. La variation inter-hospitalière observée nous indique qu’une amélioration de la qualité et de l’efficacité des soins serait possible avec les mesures appropriées.
Abstract
Background: Injury in Canada represents $27 billion in healthcare costs and 260,000 hospitalisations each year and evidence suggests that around 30% of healthcare costs could be unnecessary. Apart from representing a significant burden to the healthcare system, low-value hospitalisations can have serious consequences for patients through hospital-related adverse events and functional decline.
Objectives: To estimate the prevalence of low-value hospitalisations following injury, identify patient groups with a high prevalence of low-value hospitalisations and assess inter-hospital variation.
Methods: Using literature and expert consultation, we developed an algorithm to identify potentially low-value hospitalisations in an inclusive Canadian trauma system between April 2013 and March 2018 among patients with a primary diagnosis of injury. We then identified groups of patients with a high frequency of low-value hospitalisations. Finally, we used a multilevel robust Poisson regression model to evaluate inter-hospital variation in the prevalence of potentially low-value hospitalisations with intraclass correlation coefficients (ICC). Analyses were stratified by age (1-15; 16-64; 65-74; 75+ years).
Results: The prevalence of low-value hospitalisations was 16% (19,155/118,032) globally, 26% (2,126) in pediatric patients, 11% (4,693) in young adults and 19% (12,336) in older adults. Low-value hospitalisations were most prevalent for the following patient groups: children with mild concussion (43% of low-value pediatric hospitalisations; n=922,); young adults with superficial injuries (14%, n=660), minor spine injuries (14%, n=634) or mild concussion (11%, n=534); and older adults with superficial injuries (22%, n=2,771). We observed strong inter-hospital variation in the prevalence of potentially low-value hospitalisations (ICC=37%).
Conclusion: One out of six hospitalisations following injury may be low-value. Children with mild concussion, young adults with superficial injuries, minor spine injuries, or mild concussion as well as older adults with superficial injuries may be good targets for future research efforts seeking to reduce overuse. Inter-hospital variation indicates there may be
Introduction
In Canada, injury represents 3.5 million visits to emergency rooms and 260,000 hospitalisations per year30. Furthermore, injury care costs Canadians $27 billion per year, more than heart and stroke disease30. Evidence suggests that overuse, or the provision of
medical services for which the potential for harm exceeds the potential for benefit,
consumes around 30% of healthcare resources while reducing the quality of care given to patients3, 5. Advancing knowledge on low-value care for injury has the potential to both improve patient outcomes through a reduction in adverse events and to free up resources which can be reallocated to more appropriate care.
Research has shown that there is considerable variation in the prevalence of hospitalisations among ED presentations both between countries and between providers in the same health care system31-33, suggesting the presence of low-value hospitalisations3. Unnecessary hospitalisations are not only costly, but have negative health effects, notably through hospital-related adverse events and functional decline34-36. There is currently a major knowledge gap on low-value hospitalisations following injury.
Considering the current paradigm shift in research towards value-based healthcare, there is growing interest in identifying groups of patients which are more prone to receiving low-value care. Such data may inform research priorities and interventions seeking to reduce healthcare overuse. The objective of this study is to estimate the prevalence of potentially low-value hospitalisations following injury, identify patient groups vulnerable to low-value hospitalisations and assess inter-hospital variation.
Methods
Study Design & Population
This multicenter retrospective cohort study is based on Québec’s trauma care continuum, in which 59 designated trauma centers care for a population of over 8 million individuals over a territory of 1,356,547 km². These centers are designated level I to IV, following criteria based on the American College of Surgeons’ recommendations20
designated trauma centers provide care for approximately 20,000 injured patients each year21.
Every patient with a primary diagnosis of injury hospitalised in a designated trauma center is entered in Québec’s trauma registry. For this study, the population sample is composed of all injury hospitalisations from April 1, 2013 to March 31, 2018.
Study Data
Introduced in 1998, Québec’s trauma registry contains information on socio-demographics, injury mechanisms and diagnoses, resource use including admission service and intervention codes, as well as information on discharge destination. This database is centralized and managed by the Ministry of Health. Data quality mechanisms include standardized training for medical coders, periodic validation of the data to correct incoherence and continuous facilitated information exchange between data coders, trauma coordinators and clinical experts23.
Selection of Criteria to Identify Low-Value Hospital Admissions
We used recommendations for the design and content validation of health instruments to develop a tool to identify potentially low-value hospital admissions from the Québec trauma registry37. First, a trauma registry specialist, a trauma researcher and a trauma clinical expert used published literature17, 38-45 to select and define criteria consistent with patients not requiring hospitalisation. Second, 8 experts (2 emergency physicians, 2 critical care physicians, a trauma surgeon, a general practitioner, a trauma care co-ordinator, and a trauma system manager) were individually consulted to validate the relevance and content of each criteria. Third, criteria were applied to trauma registry data and an age-stratified random sample of patient records were extracted and revised by the same experts to refine criteria. This last step was repeated three times until no further modifications were suggested. Examples of modifications are a more exhaustive list of interventions not requiring hospital admission and the exclusion of criteria on comorbidities due to the lack of information on their severity. The final tool included 6 criteria (supplemental digital content 1).
Statistical Analysis
In order to identify patients groups with a high frequency of potentially low-value hospitalisations, patients were stratified by age group (1-15, 16-64, 65-74, 75+) and primary diagnosis.
To evaluate inter-hospital variation in the prevalence of low-value hospitalisations, we used a multilevel robust Poisson regression model to generate intraclass correlation coefficients (ICC). ICC measures the percent variation in low-value hospitalisations between hospitals which is not explained by patient case mix. Inter-hospital variation was considered to be weak, moderate and strong for ICC under 5%, between 5% and 20%, and over 20%, respectively27. We adjusted for casemix using age (1-4, 5-12, 13-15, 16-54, 55-64, 65-74, 75-84, 85+), sex, the New Injury Severity Score (1-3, 4, 5-6, 8-11, ≥12), the Glasgow Coma Scale score (≤13, 14, 15), injury mechanism (motor vehicle collision, fall from height, fall from own height, penetrating injury, other), number of injuries (1, 2, 3+), primary injury diagnosis and number of comorbidities. Analyses were conducted for the whole sample and according to age (1-15, 16-64, 65-74, 75+).
The Glasgow coma scale score was missing for 50% of our study population. This is because physicians often do not evaluate level of consciousness in patients with minor, extracranial injury. This issue was addressed using multiple imputation, a method in which a predictive model is used to simulate multiple values based on correlated variables. Glasgow coma scale score was predicted using age, sex, injury severity, injury mechanism, number of injuries, type of injury and comorbidities. We generated 50 imputations, based on the percent of missing information 46.
All analyses were performed using Statistical Analysis Software (SAS Institute, Cary, NC, version 9.4). The study was approved by the research ethics committee of the CHU de Québec – Université Laval.
Sensitivity analyses
We conducted sensitivity analyses successively removing patients in whom hospitalisation may have been justified from the numerator. First, we removed patients who developed
complications during their stay. Second, we removed patients who had a GCS of 13 or 14 on arrival. Third, we removed patients with a discharge destination involving additional medical attention (for example patients discharged home with service or to care homes). Finally, we removed patients who were transferred-in from another hospital. In all cases, patients were removed from the numerator but not from the denominator (patients were no longer considered low-value hospitalisations). For each sensitivity analysis, we compared the prevalence of low-value hospitalisations and inter-hospital variation (ICC).
Results
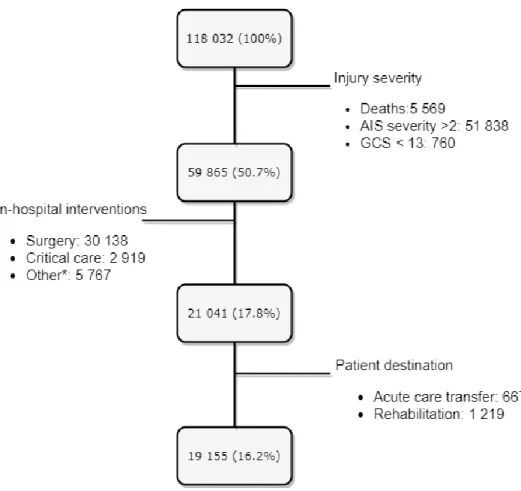
After excluding patients who died, had severe injuries, a Glasgow Coma Scale score under 13, received a clinical intervention for which hospitalisation was required (detailed in supplemental digital content 1), needed rehabilitation, or were transferred to an acute care center, our final sample of potentially low-value hospitalisations comprised 19,155 (16%) patients (Figure 1). This proportion varied by age group from 11% in young adults to 26% in children.
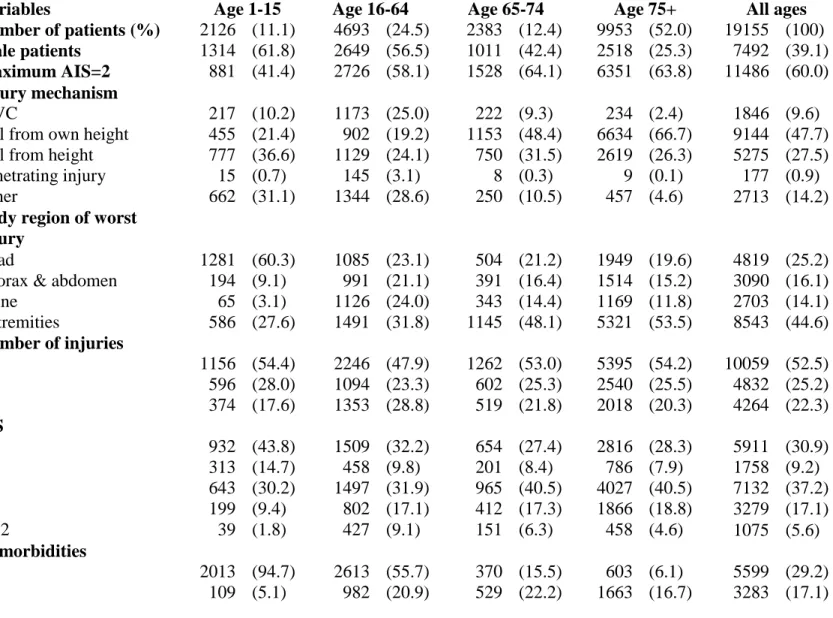
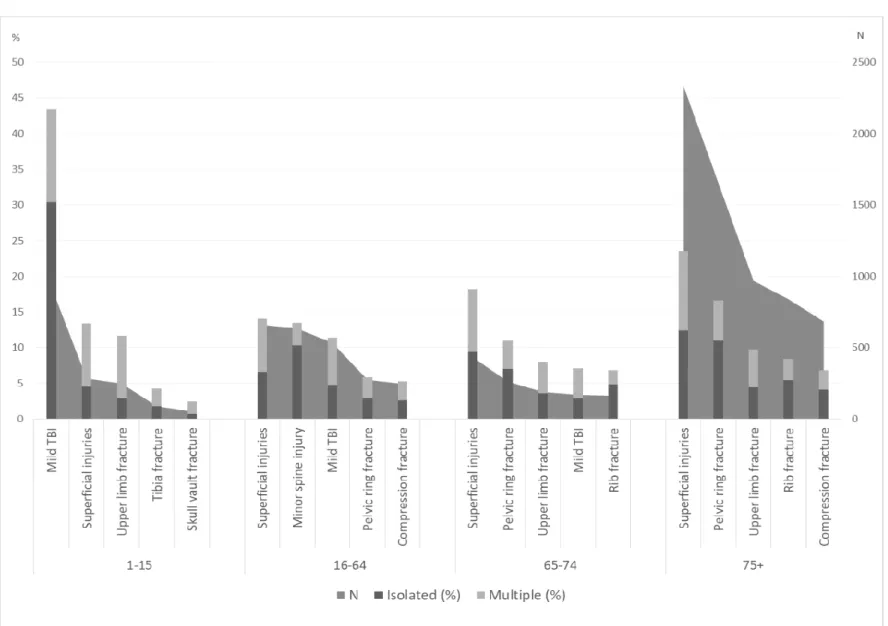
Overall, 64% of patients were aged 65 or more, 39% were male, 60% of patients had a maximum Abbreviated Injury Scale (AIS) of 2, 50% had isolated injuries, falls were the most common injury mechanism and most patients were treated in a level III trauma center (Table 2). Over half of patients had only one injury, 45% of injuries were to extremities, and 25% of injuries were to the head. The proportion of male patients decreased with age and while fall from height was the common mechanisms for patients <65 years of age, falls from standing height was most common in patients ≥65. Children more often had less severe injuries (59% with AIS=1 compared to 40% in adults), head injuries (60% compared to 20% in adults) and were more often transferred-in (16% compared to 6% in adults). Based on age group and primary diagnosis, potentially low-value hospitalisations were most prevalent in the following groups: children with mild concussion (922; 43% of low-value pediatric hospitalisations); young adults with superficial injuries (660; 14%), minor spine injuries (634; 14%) or mild concussions (534; 11%); or older adults with superficial injuries 2,771; 22%) (Figure 2).
Out of the 19,155 patients with a low-value hospitalisation, 5,582 (29%) received at least one therapeutic intervention in the emergency department (Figure 3). Only 3,471 (18%) patients received one or more therapeutic intervention following hospitalisation, and over 80% of these were administrations of antithrombotic agents. Administration of medication was the most common therapeutic intervention in every patient group, except those diagnosed with an extremity fracture in whom reductions and immobilizations were more frequent.
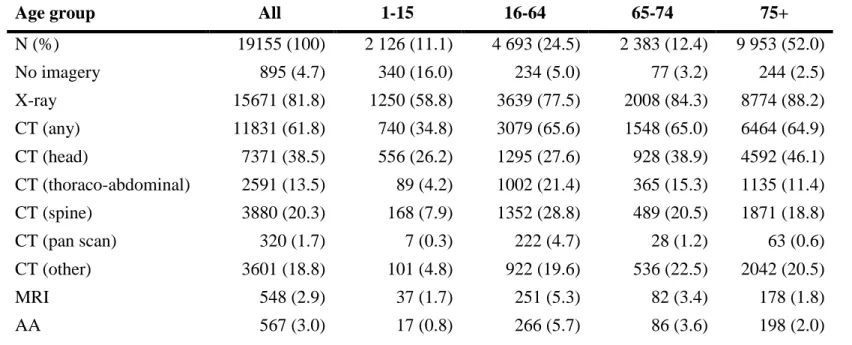
Concerning imaging, 17,682 (92%) patients received at least one imaging procedure (Table 3). X-ray was used in over 80% of patients in every age group except children (56%). Head CT was the predominant advanced imagery modality used in every age group (39% of patients).
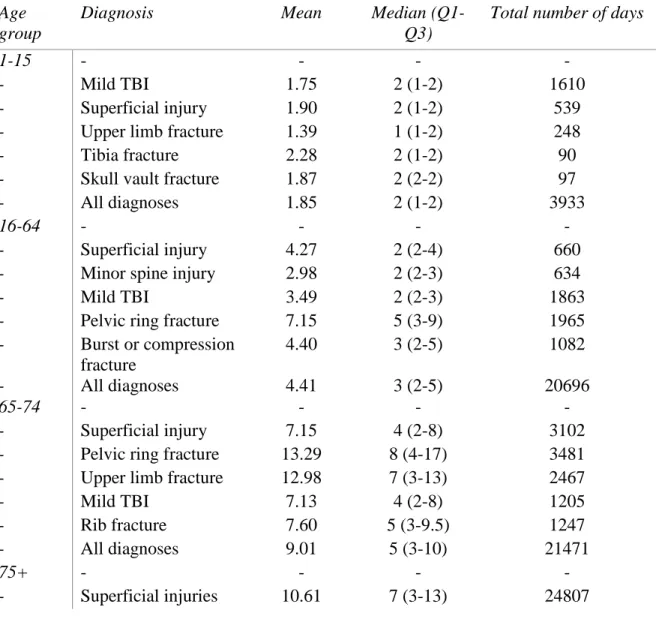
Length of stay was shorter in children with a median at 1 or 2 days depending on diagnosis and longer in adults 75 years of age or older, with a median varying from 7 to 13 days depending on diagnosis (Table 4). Our population of potentially low-value injury hospitalisations in the Québec trauma system accrued on average 36,073 days of hospitalisation per year.
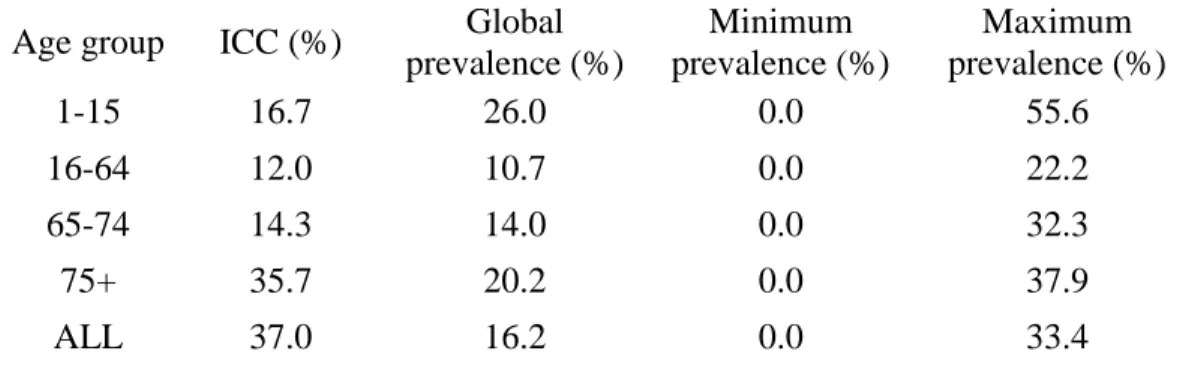
We observed strong variation in the prevalence of potentially low-value hospitalisations between hospitals with an ICC=37% (prevalence between 0% and 33%) (Figure 4). When we stratified by age, inter-hospital variation remained strong for patients over 74 years of age and was moderate for every other age group (Table 5). Even within designation levels, variation remained high with prevalence varying between 10% and 23% for level I and II trauma centers. However, higher level centers had lower average prevalences than lower level centers.
Sensitivity analyses
Most of the sensitivity analyses had little impact on the results (Table 6). When patients with a GCS of 13 or 14, or patients who developed an in-hospital complication were removed from the numerator, prevalences and ICC all varied by less than 10%. The removal of transferred-in patients had an impact on children, which were the group in which the most transfers were observed (prevalence of 22% compared to 26%). Finally, the
analysis which had the most impact was that for which we removed any patients who were provided extra services on discharge (e.g. home with help, care home). However, even in the most impactful sensitivity analysis, the ICC remained over the threshold for strong variation.
Discussion
In this multicenter retrospective cohort study, 16% of all injury hospitalisations in a Canadian trauma system were considered potentially low-value. Patient groups with a high frequency of potentially low-value hospitalisations were children with mild concussion, young adults with superficial injuries, minor spine injuries or mild concussions, and older adults with superficial injuries. We observed strong inter-hospital variation in potentially low-value hospitalisations (ICC=37%).
Our results show a concentration of potentially low-value hospitalisations in children with head injuries. This is consistent with many other studies observing high prevalence of admission for observation among children with head injuries despite extremely low rates of missed injuries following diagnosis in these patients17, 40, 41, 47-52. This over-representation of children with head injuries is sometimes attributed to the fact that some physicians are less experienced in treating pediatric patients and are afraid of potentially life-threatening missed intracranial injuries53, 54. The high prevalence of potentially low-value hospitalisations in children may also be related to the high number of transferred patients in this group, who are more likely to be admitted than patients presenting directly to the ED. Only 2 of the 59 designated trauma centers in our population are specialized in pediatric trauma care, and 38% of potentially low-value hospitalisations in those 2 centers were children transferred-in from another acute care hospital.
Young adults (16-64 yoa) are the group with the lowest prevalence of potentially low-value hospitalisations. It is also the group with the most varied injuries, with none of the primary diagnoses representing more than 14% of hospitalisations in this group. This group has the highest frequency of motor vehicle collisions, which may lead to potentially low-value hospitalisations; this mechanism is often used as a triage criteria because of its potential for
explain potentially low-value admissions in this group, since it is the group in which substance abuse is most prevalent and intoxicated patients pose a challenge in terms of diagnostic evaluation, notably for TBI and spine injuries56, 57.
Patients aged 65 years and over composed 64% of the potentially low-value hospitalisations in our sample. Research has shown this patient group is particularly complex to care for since many of them have difficulties with mobility or communication, or develop delirium, all of which may lead to longer lengths of stay58. They are also more susceptible to hospital related adverse events caused by longer lengths of stay such as functional decline or nosocomial infections, which often exacerbate the problem and lead to additional hospital days 6, 59. Delayed discharge due to problems accessing post-acute care is also a problem in this patient group 60, 61.
We observed strong inter-hospital variation in the prevalence of potentially low-value hospitalisations, but more specialized trauma centers, in general, had a lower prevalence than level III and IV centers. A potential explanation is that physicians working in centers with a higher volume of injury presentations have a better understanding of whether or not patients require hospitalisation. This may also be due to bed availability, which could be less of an issue in rural hospitals due to low patient volume.
Other potential determinants of low-value hospitalisations include lack of interdisciplinary services consultation in the ED, particularly for the elderly, who may be hospitalised for evaluation before decisions concerning discharge can be made62. On a similar note, potentially low-value hospitalisations may be due to lack of resources; smaller hospitals which do not have equipment such as CT scans may need to hospitalize more patients for observation. Finally, low-value hospitalisations may be largely driven by resources available to the patient at home or in the community. Patients living alone who have an injury restricting mobility may have to be admitted while alternative care is secured.
Both in the ED and after hospitalisations, most patients (71% and 82% respectively) did not receive any therapeutic intervention (Figure 3), possibly highlighting the low utility of these hospitalisations. In addition, interventions were mostly reductions, immobilisations or
administrations of analgesics or antithrombotics that may have been administered in the ED or even at home.
Although few patients received a therapeutic intervention, most patients received a radiographic evaluation and/or a CT scan. This is consistent with estimates of overuse of imaging for ED patients, notably for minor head trauma63. This represents a considerable amount of time and resources invested in patients which may not have needed imaging and also represents radiation exposure which, depending on the age of the patient, could have long-term consequences16.
Strengths and limitations
This study has several strengths. We had access to high-quality, current clinical data which, contrary to hospital discharge data, has detailed information on physiological reaction to injury (e.g. GCS and systolic blood pressure on arrival) and anatomical injury severity. Furthermore, unlike many trauma registries that condition inclusion on injury severity, the Québec registry includes all hospitalisations for injury in any designated trauma center. Since the definition we used for low-value care was not validated, we were not able to identify patients in which hospitalisations could be definitively considered as low-value. Because of this limitation, we instead sought to use broad filters in order to identify
potentially low-value hospitalisations to find trends that could help further research on the
subject. In addition, considering the secondary and retrospective nature of our data, our study is subject to potential measurement error and missing data (50% for the GCS). There is a possibility that hospitals with a low prevalence of low-value hospitalisations are undertriaging patients in which hospitalisation was required. However, we consider this unlikely as highly specialized, high-volume centers in which undertriage is more likely tended to have a lower prevalence than lower-level centers in our sample. We did not exclude patients based on comorbidities as we had no information on their severity and most patients over 65 had at least one comorbidity, which may be well-controlled and not related to admission.
This study does not include patients admitted to non-designated trauma centers, which a study estimated to represent 25% of injury hospitalisations for all trauma and is likely to represent a much higher percentage for minor injury22. This likely means we have a selection bias towards patients with more severe injuries since these require the expertise of designated centers. Considering this, we expect our results to underestimate the prevalence and costs of low-value hospitalisations because non-designated centers may be less comfortable with discharging patients from the ED, even for minor injuries.
There may also be measurement error among variables used to adjust inter-hospital comparisons. For example, comorbidities could be underestimated or very minor injuries may not always be reported. This could lead to an overestimation of the inter-hospital variation of low-value hospitalisations. We may also have omitted potential confounders, such as patient mobility, pain, socio-economic status and social support, because they were not available in the registry. These variables may influence decisions regarding discharge. Finally, the registry does not contain information on patients which were returned home from the ED so we could not compare patients admitted to those who were not.
Impact and future research
Further research will be required in order to fully assess whether identified hospitalisations truly represent low-value care. Thereafter, research will also be necessary to determine whether low-value hospitalisations could be reduced by interventions optimizing care in the ED or in the community. If even a fraction of these hospitalisations truly represent overuse, a modification of care processes in this population has the potential to free up resources as well as improving the clinical outcome of patients.
Older adults are of particular interest, on one hand their complexity and fragility makes it harder to adequately modify practices to try and reduce the amount of care given to them. But on the other hand, they are a group in which such modifications could yield considerable gains both in terms of resources saved and improved outcomes since they have a high risk of functional decline and other hospital-related adverse events6, 59.
Conclusion
In the inclusive trauma system of Québec, we estimated one out of six hospitalisations following injury may be low-value. Children with mild concussion, young adults with superficial injuries, minor spine injuries, or mild concussion as well as older adults with superficial injuries may be good targets for future research efforts seeking to reduce overuse. Strong inter-hospital variation indicates that low-value hospitalisations may have the potential to be reduced with appropriate interventions.
Figure 1. Algorithm to select potentially low-value hospitalisations
*Other interventions include all interventions except those considered not to require hospitalisation (Supplemental digital content 1)
Table 2. Description of the study population
Variables Age 1-15 Age 16-64 Age 65-74 Age 75+ All ages
Number of patients (%) 2126 (11.1) 4693 (24.5) 2383 (12.4) 9953 (52.0) 19155 (100)
Male patients 1314 (61.8) 2649 (56.5) 1011 (42.4) 2518 (25.3) 7492 (39.1)
Maximum AIS=2 881 (41.4) 2726 (58.1) 1528 (64.1) 6351 (63.8) 11486 (60.0)
Injury mechanism
MVC 217 (10.2) 1173 (25.0) 222 (9.3) 234 (2.4) 1846 (9.6)
Fall from own height 455 (21.4) 902 (19.2) 1153 (48.4) 6634 (66.7) 9144 (47.7) Fall from height 777 (36.6) 1129 (24.1) 750 (31.5) 2619 (26.3) 5275 (27.5)
Penetrating injury 15 (0.7) 145 (3.1) 8 (0.3) 9 (0.1) 177 (0.9)
Other 662 (31.1) 1344 (28.6) 250 (10.5) 457 (4.6) 2713 (14.2)
Body region of worst injury
Head 1281 (60.3) 1085 (23.1) 504 (21.2) 1949 (19.6) 4819 (25.2)
Thorax & abdomen 194 (9.1) 991 (21.1) 391 (16.4) 1514 (15.2) 3090 (16.1)
Spine 65 (3.1) 1126 (24.0) 343 (14.4) 1169 (11.8) 2703 (14.1) Extremities 586 (27.6) 1491 (31.8) 1145 (48.1) 5321 (53.5) 8543 (44.6) Number of injuries 1 1156 (54.4) 2246 (47.9) 1262 (53.0) 5395 (54.2) 10059 (52.5) 2 596 (28.0) 1094 (23.3) 602 (25.3) 2540 (25.5) 4832 (25.2) 3+ 374 (17.6) 1353 (28.8) 519 (21.8) 2018 (20.3) 4264 (22.3) ISS 1 932 (43.8) 1509 (32.2) 654 (27.4) 2816 (28.3) 5911 (30.9) 2-3 313 (14.7) 458 (9.8) 201 (8.4) 786 (7.9) 1758 (9.2) 4 643 (30.2) 1497 (31.9) 965 (40.5) 4027 (40.5) 7132 (37.2) 5-6 199 (9.4) 802 (17.1) 412 (17.3) 1866 (18.8) 3279 (17.1) 8-12 39 (1.8) 427 (9.1) 151 (6.3) 458 (4.6) 1075 (5.6) Comorbidities 0 2013 (94.7) 2613 (55.7) 370 (15.5) 603 (6.1) 5599 (29.2) 1 109 (5.1) 982 (20.9) 529 (22.2) 1663 (16.7) 3283 (17.1)
2 4 (0.2) 553 (11.8) 534 (22.4) 2418 (24.3) 3509 (18.3)
3+ 0 (0) 545 (11.6) 950 (39.9) 5269 (52.9) 6764 (35.3)
Trauma center level 0
I 576 (27.1) 648 (13.8) 214 (9.0) 1040 (10.5) 2478 (12.9)
II 200 (9.4) 776 (16.5) 374 (15.7) 1566 (15.7) 2916 (15.2)
III 1176 (55.3) 2793 (59.5) 1452 (60.9) 6028 (60.6) 11449 (59.8)
IV 174 (8.2) 476 (10.1) 343 (14.4) 1319 (13.3) 2312 (12.1)
Table 3. Imagery use by age group in potentially low-value hospitalisations
Age group All 1-15 16-64 65-74 75+
N (%) 19155 (100) 2 126 (11.1) 4 693 (24.5) 2 383 (12.4) 9 953 (52.0) No imagery 895 (4.7) 340 (16.0) 234 (5.0) 77 (3.2) 244 (2.5) X-ray 15671 (81.8) 1250 (58.8) 3639 (77.5) 2008 (84.3) 8774 (88.2) CT (any) 11831 (61.8) 740 (34.8) 3079 (65.6) 1548 (65.0) 6464 (64.9) CT (head) 7371 (38.5) 556 (26.2) 1295 (27.6) 928 (38.9) 4592 (46.1) CT (thoraco-abdominal) 2591 (13.5) 89 (4.2) 1002 (21.4) 365 (15.3) 1135 (11.4) CT (spine) 3880 (20.3) 168 (7.9) 1352 (28.8) 489 (20.5) 1871 (18.8) CT (pan scan) 320 (1.7) 7 (0.3) 222 (4.7) 28 (1.2) 63 (0.6) CT (other) 3601 (18.8) 101 (4.8) 922 (19.6) 536 (22.5) 2042 (20.5) MRI 548 (2.9) 37 (1.7) 251 (5.3) 82 (3.4) 178 (1.8) AA 567 (3.0) 17 (0.8) 266 (5.7) 86 (3.6) 198 (2.0)
Table 4. Length of stay by age and diagnosis in potentially low-value hospitalisations
Age group
Diagnosis Mean Median
(Q1-Q3)
Total number of days
1-15 - - - -
- Mild TBI 1.75 2 (1-2) 1610
- Superficial injury 1.90 2 (1-2) 539
- Upper limb fracture 1.39 1 (1-2) 248
- Tibia fracture 2.28 2 (1-2) 90
- Skull vault fracture 1.87 2 (2-2) 97
- All diagnoses 1.85 2 (1-2) 3933
16-64 - - - -
- Superficial injury 4.27 2 (2-4) 660
- Minor spine injury 2.98 2 (2-3) 634
- Mild TBI 3.49 2 (2-3) 1863
- Pelvic ring fracture 7.15 5 (3-9) 1965
- Burst or compression fracture 4.40 3 (2-5) 1082 - All diagnoses 4.41 3 (2-5) 20696 65-74 - - - - - Superficial injury 7.15 4 (2-8) 3102
- Pelvic ring fracture 13.29 8 (4-17) 3481
- Upper limb fracture 12.98 7 (3-13) 2467
- Mild TBI 7.13 4 (2-8) 1205
- Rib fracture 7.60 5 (3-9.5) 1247
- All diagnoses 9.01 5 (3-10) 21471
75+ - - - -
- Pelvic ring fracture 17.52 13 (7-13) 28946
- Upper limb fracture 13.86 9 (5-18) 13414
- Rib fracture 13.45 9 (5-17) 11283
- Burst or compression fracture
15.22 12 (6-20) 10394
- All diagnoses 13.49 9 (4-17) 134265
Figure 4. Adjusted prevalence of potentially low-value hospitalisations by hospital and trauma center designation level 0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45 0 5 1 0 1 5 2 0 2 5 3 0 3 5 4 0 4 5 5 0 5 5 Prev alence (% ) Hospital
Table 5. Sub-group analysis: inter-hospital variation by age group
Age group ICC (%) Global
prevalence (%) Minimum prevalence (%) Maximum prevalence (%) 1-15 16.7 26.0 0.0 55.6 16-64 12.0 10.7 0.0 22.2 65-74 14.3 14.0 0.0 32.3 75+ 35.7 20.2 0.0 37.9 ALL 37.0 16.2 0.0 33.4
Table 6. Sensitivity analyses
Prevalence of potentially low-value hospitalisations (%) ICC (%)
Age group All 1-15 16-64 65-74 75+ All
Main analysis 16.2 26.0 10.8 14.0 20.2 36.9
Complications1 13.8 25.8 10.1 12.1 15.6 35.4
GCS2 15.9 24.8 10.6 13.9 19.8 36.7
Discharge3 6.1 17.4 6.6 5.6 3.9 29.9
Transfers4 15.3 21.8 9.8 13.3 19.7 36.1
1: Patients with complications removed from the numerator 2: Patients with a GCS of 13 or 14 removed from the numerator
3: Patients who were discharged with extra services provided from the numerator 4: Patients transferred-in removed from the numerator
Supplemental digital content 1. Criteria for identifying low-value hospital admissions
Patients meeting all of the following criteria were considered as low-value admissions: 1. Minor injury:
Maximum Abbreviated Injury Scale score ≤2) 2. Normal neurological status:
Glasgow Coma Scale ≥13 on arrival at the ED and on admission
3. No intervention (other than diagnostic imaging) considered to require hospital admission, i.e. no interventions other than the following:
Percutaneous administration of antiinfective
Percutaneous administration of antithrombotic agent Percutaneous administration of analgesic
Shoulder joint percutaneous administration of corticosteroids Hip joint percutaneous administration of corticosteroids Knee joint percutaneous administration of corticosteroids Knee joint local administration of anesthetic agent
Spinal canal and meninges percutaneous transcatheter administration of analgesic agent
Radius and ulna reduction using closed approach Humerus immobilization using cast
Shoulder joint immobilization using cast Wrist joint immobilization using cast Tibia and fibula immobilization using cast Ankle joint immobilization using cast Radius and ulna immobilization using cast Foot immobilization using cast
Ankle joint immobilization using pneumatic orthotic device (air cast) Knee joint immobilization using splinting device
Skin of abdomen and trunk – using occlusive dressing Hemodialysis
Humerus immobilization using splinting device
Ankle joint immobilization using pneumatic orthotic device (air cast)
Radius and ulna reduction using closed approach 4. Alive on discharge
5. Discharge destination not indicative of requiring further acute care: Home
Nursing home
Long-term care facility
Chapter V. Discussion
5.1 – Summary of results in line with objectives
To our knowledge, this is the first study to estimate the prevalence of low-value hospitalisations in an inclusive trauma system. Overall, 16% of all injury hospitalisations in a Canadian trauma system were considered potentially low-value. Low-value hospitalisations were most frequent in children (26%) and older adults (19%) but still constituted 11% of hospitalisations in young adults. Low-value hospitalisations were most prevalent for the following patient groups: children with mild concussion (43% of low-value pediatric hospitalisations; n=928,); young adults with superficial injuries (14%, n=661), minor spine injuries (14%, n=634) or mild concussion (11%, n=534), and older adults with superficial injuries (22%, n=2,774). We also observed strong inter-hospital variation (37%) in potentially low-value hospitalisations, highlighting a potential for improvement. The sub-group analysis showed that the ICC varied between age groups, ranging from 12% in young adults to 36% in patients over 74 years of age. Although some of these sub-group ICCs vary considerably from the global estimate, all of them still represent moderate to strong variation and a lower ICC is to be expected in more homogenous groups.
5.2 – Comparison with the literature
The prevalence of potentially low-value hospitalisations varied by age and went from 11% to 26%. One study of potentially inappropriate admissions observed prevalences of low-value use of acute care beds of 6% to 28% depending on the indicator used64. Choosing Wisely Canada also found up to 30% unnecessary tests treatments among procedures for which they emitted recommendations63. Studies also demonstrate that age is determinant of low-value care33, 64. A 2016 study found younger age to increase the chance of being unnecessarily admitted to a surgical ward, and older adults are known to have higher rates of hospitalisations for preventable conditions64, 65. Mild TBI was among the most frequent diagnoses for children and young adults in our sample, representing over 40% of primary diagnoses in children. These results are in line with the fact that many authors claim hospitalisations for observation in cases of mild TBI are common despite very low rates of
missed injuries following diagnosis in these patients17, 40, 47, 48. The most frequent primary diagnosis in older adults was superficial injuries. This is consistent with a Canadian study which looked at acute health care use in older adults, in which contusions were the most common injury66. The potential causes of low-value hospitalisations vary with age. In children, some authors suggest that physicians who are not specialized in paediatrics may be hesitant to discharge children from the ED, which leads to frequent admissions for observation53, 54. This is reflected in the high proportion of transfers we observed in children (16%) and may lead to low-value hospitalisations since children transferred-in from another hospital are more likely to be hospitalised. Young adults more often present to the ED intoxicated than other age groups; these patients are known to be challenging to evaluate, which can lead to low-value hospitalisations56, 57. They are also the group with the most motor vehicle collisions as their injury mechanism. This mechanism is sometimes used as a triage criterion due to its potential for severe injuries but is known to lead to overtriage55. In older adults, despite the fact that trauma registry inclusion criteria state that injury should be the primary reason for the hospitalisation, pre-existing conditions are likely to have influenced the decision to hospitalize in our patient population 58. The inter-hospital variation observed in our study is consistent with studies demonstrating considerable variation in hospitalisation rates among ED presentations between hospitals and between systems in other patient populations31-33.
5.3 – Internal validity
5.3.1 – Selection bias
In our study, the fact that around 25% of injured patients are treated in hospitals that are not designated trauma centers may represent a selection bias since these patients are not included in Québec’s trauma registry22. A selection bias will be present if the patients treated outside the trauma system differ from those treated in the system. It is safe to assume that most injuries treated in non-designated trauma centers are minor since pre-hospital protocols and inter-pre-hospital transfer agreements aim to transport patients with major trauma to designated trauma centers. It is also possible that physicians in non-designated centers are less comfortable discharging minor trauma from the ED.
Considering this, we believe we underestimated the prevalence of low-value hospitalisations. We could have used hospital discharge data to obtain information on all hospitalisations. However, this database does not contain information on injury severity or physiological reaction to injury.
5.3.2 – Information bias
The categorization of potentially low-value hospitalisations in our study exposes it to a potential information bias since we did not use a validated definition. In addition, some variables used to identify potentially low-value hospitalizations may have been subject to measurement error. If coding errors vary across hospitals, this information bias may be differential. In each case, this could cause an underestimation or an overestimation of the prevalence. However, multiple mechanisms have been put in place to ensure the quality and standardization of trauma registry data23.
5.3.3 – Confusion bias
There are two potential sources of residual confounding in our study; variables which are subject to measurement error or variables which are not available in the trauma registry. For example, comorbidities are known to be underreported in trauma registries, which could cause us to overestimate inter-hospital variation. This problem may vary between centers and between designation levels. Concerning unavailable variables, since this is a secondary data analysis and we could not handpick which variables were available to us, some variables which could have been used in the adjustment of the model or to identify the potentially low-value hospitalisations were unavailable. These mostly regard the status of the patient before their arrival at the hospital. Characteristics such as the socio-economic status of the patient and their social net, or their functional status and the amount of care which is provided to them in their residence could help inform difficulties in returning these patients home. We also had no information on pain or control of pain which could also influence the decision to discharge from the ED which could have led to an overestimation of the prevalence of low-value hospitalisations.
5.4 – External validity
The results of this study may be applicable in similarly organized trauma systems such as other Canadian provinces, the United Kingdom or Australia, but not in non-universal systems such as the United States. However, differences in pre-hospital and community care, and differing availability of primary care, hospital beds, and services in the ED, may make comparisons between systems difficult.
6.0 – Conclusion
This study suggests that low-value hospitalisations are a prevalent problem in our trauma system, and therefore that interventions targeting their reduction have the potential to improve resource utilization and patient outcomes. It has also highlighted groups of patients in which such interventions could prove particularly fruitful. In addition, this study provides a method to measure potentially low-value hospitalisations, which may be applied to other populations. This would allow for comparisons not only between centers within a trauma system but also across different systems, which could lead to the identification of further strategies to reduce low-value care. More research will be required to establish whether these hospitalisations really represent low-value care, for example using expert case review. Future research on low-value hospitalisations should focus on refining their definition and pinpointing their root causes. Once these causes are identified, solutions will need to be developed, implemented, and their effectiveness evaluated.