Vaginoplasty Using
Amniotic Membranes
in
Cases of
Vaginal Agenesis
or
after
Vaginectomy
MICHELLE
NISOLLE,
M.D.,
andJACQUES DONNEZ,
M.D.,
Ph.D.
ABSTRACT
Various
treatments havebeen
proposed
for
vaginal
agenesis.
The authors describe successful
procedures using
amniotic
membranes
as agraft
onvaginoplasties.
The amnion
was notstripped
from
thechorion. The results showed the
vagina
tobe well formed
andof normal
depth
and caliber.
(J
GYNECOL SURG
8:25, 1992)
INTRODUCTION
Malformations
of the vagina are an uncommon but seriousproblem.
Theirseverity
ranges fromcomplete vaginal agenesis,
withorwithoutfunctioning
uterus, tovaginal shortening.
The treatment of certain
gynecologic malignancies,
such asvaginal
adenocarcinoma orvaginal
severedysplasia
inducedby
DES,
requires
vaginectomy,
which makes coitusimpossible.
Insomeinstances,
radicalhysterectomy
forseverecervicaldysplasia
mustbe associated withvaginectomy
because of the presence ofassociated
vaginal dysplasia.
Vaginal
constructionorreconstruction hasbecomeawell-established methodtopermit
orrestoresexualfunction,
andavariety
ofprocedures
have been described. Themostpopular
method involveslining
asurgically
created space, either withapartial
thickness skingraft'
orwithamnion.2-10
In
1934,
Brindeau2
used human amnion to construct thevagina
for apatient
with mullerianagenesis.
Between 1939 and
1947,
Burger3
usedamnionmoreextensively
for the samepurpose. In1973,
Trelfordetal.7
successfully
used fetal amnionto reconstructthevagina during
anteriorexenteration.Inour
study,
amniotic membranes have been usedtoline theartificially
constructedvagina.
The authorsreport
theirexperience
with theuseof amniotic membranes.PATIENTS AND
METHODS
Between 1986 and
1990,
amniotic membraneswereused in 10patients undergoing vaginoplasty
for variousetiologies,
shown in Table 1.The age of the
patients ranged
between 14 and 59 years.Thesametechnical
procedure
ofvaginoplasty
wasused for the 6patients suffering
fromvaginal agenesis.
None of them had
undergone
avaginoplasty anteriorly.
Amniotic membraneswere
placed
into theneovagina
created incasesofvaginal agenesis
(n
=6)
orinto thevesicorectal space
remaining
aftervaginectomy
(n
=4).
Under
general
anesthesia,
thepatient
wasplaced
in thelithotomy
position,
and thevaginal
dissectionwasperformed.
Avaginal pouch
wascreatedby
bluntdissection,
with thehelp
of scissors. At thesametime,
alaparoscopy
wascarriedout toconfirm thediagnosis
and check the blunt dissection. When hemostasis had beenachieved,
avaginal
mold(Fig.
1)
wasselected ofasizejust large enough
toensurefirmapplication
of theInfertility
ResearchUnit,CatholicUniversity
ofLouvain, Brussels,Belgium.
Table 1. TypeofVaginal Abnormalityand PostoperativeFunctional Results
Vaginal length
(cm)Etiology
of
vaginoplasty
Preoperative
Postoperative
Functional resultsVaginal agenesis
(n =6)
(Rokitansky-Kuster-Hauser
syndrome)
Vaginal malignancy
(n =4)
Vaginal
adenocarcinoma(post-DES
exposure)
(n = 1)Vaginal epidermoid
carcinoma (n = 3)1 1 I I 1 3
Vaginectomy
andhysterectomy
Vaginectomy
andhysterectomy
+ + +-+ +-++c + ++c + ++c + ++c + ++c + ++c +++c + ++c b"No sexual intercourse.
Only
the mold is used. bFailurebecause of insufficient motivation.cNormal
vaginal capacity.
amniotic
membranes,
with which it wascovered. The labiamajora
wereapproximated
with silk sutures tokeep
the mold inplace.
AFoley
catheterwasinserted before the blunt dissection and left for 48 hours. Aftervaginectomy,
simultaneously
performed abdominally
andperineally,
the space between the bladder and the rectumwasused forapplication
ofthe mold.The membranesweretaken
immediately
postpartum
fromaseronegative patient
who hadbeen afebrile andwhose membranes had been
ruptured
for less than 6 hours. In allcases,delivery
occurred 3to6 hoursbeforevaginoplasty. Delivery
wasvaginal
inall cases. Electivecesarean sectionwasnotacondition foruseof themembranes. The membranesarerinsed insterile saline solutiontoremoveall the blood and storedat4°Cin
asaline solution
(without
anyantibiotic).
Inoursurgical procedure,
amnioticmembraneswereused,
and theamnion wasnot
stripped
from the chorionbeforeitsuse.The mold
wrapped
inamnioticmembraneswasinserted. Two silksuturesin the labiamajora
maintained the mold inposition.
The entireprocedure
wascompleted
in 20 minutes. Allpatients
weregiven
antibioticsfor 6to7
days postoperatively.
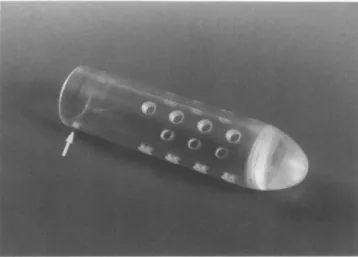
FIG. 1.
Rigid vaginal
mold(diameter3.5cm,length
10or12cm).The holes allow thedrainage
ofvaginal
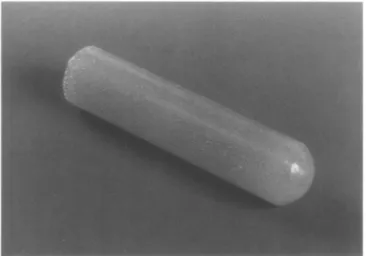
exudations.FIG. 2.
Nonrigid vaginal
mold(diameter3.5cm,length
10or12cm).Themoldwasremoved under
light
sedation7days
later,
andthenewly
constructedvagina
wasinspected
and cleaned. The amniotic membranes were found adherent to the
vagina.
Anonrigid
mold(Fig.
2)
wasinserted,
and thepatient
wasdischarged
thefollowing
day
and advisedtorefrain from sexualactivity
foranadditional 2 weeks andtousethe moldat
night during
thisperiod.
Dienestrolcreamwasusedas alubricant.The
patient
thenwasencouraged
tohavesexual intercourse. Allpatients
werereviewed 2 weeks and 1 monthpostoperatively
and thenatmonthly
intervals.RESULTS
All
patients
found the molduncomfortablepostoperatively,
but allweremobile andrequired
mildanalgesia
only
for the moldchange
onthe seventhday.
Routineurinary
catheter insertionwasperformed
inallpatients
for 48 hours. All
patients
receivedprophylactic
antibiotics,
penicillin
and metronidazole. Nopatient
developed
aurinary
tractinfection. At themoldchange,
the amniotic membranes could beseenasadistinctlayer applied
tothevaginal
wall. At the endofthe 7days,
thevaginal
tunnelwascovered withasmoothlining
with
widespread
but small areasofcongestion.
By
the fourth weekpostoperatively, healthy pink vaginal epithelium
wasvisiblewith,
insomecases,only
smallareasof
granulation
tissue. Initialepithelialization
wasexcellent. At the end of the 8weeks,
thevagina
wasfoundtobe well formed andwasofnormal
depth
and caliber. Therewere noadhesions, exúdate,
drying,
orscarring.
Constantuseof the mold didnotresult inaninflammatory
reactionwith formation ofagranuloma
in unmarried
patients.
Therectumwasnotentered in any
patient during
vaginal
dissection.All
patients
were reviewed 2 weeks and 1 monthpostoperatively
and thenatmonthly
intervals.Vaginal
smears at 8 weeks
postoperatively
showed numerous squamousepithelial
cells. In all cases ofvaginal
agenesis,
except
one,epithelialization
wascomplete,
asproved by biopsy,
which showedearly
epithelializa-tion
(at
week4-6)
andmaturevaginal
epithelium by
the end of 8to10weeks(Fig.
3).
Inonecase,granulation
tissuewasfound,
estrogen
vaginal
cream wasnotusedby
thepatient.
Incasesofvaginectomy
forgynecologic
malignancies, epithelialization
tooklonger,
about 2to3 months.The anatomic andfunctionalresultsaresummarizedin Table 1. The
length
of thevagina
wasfoundtovaryfrom7 to8cm. All
patients
hadgreatly
improved
vaginal length
andcapacity
as aresult ofthistreatment. Excellent results wereachieved in allcasesexcept
one. The oldestpatient
discontinued theuseof the moldafter
leaving hospital.
Two weekspostoperatively,
therewascomplete
vaginal
closure. Thisfailurecould beexplained by
insufficient motivation of thepatient.
In the othercases,thevaginal
tissue remainedsupple,
withnoevidence of fibrous tissue formation. Chronic
granulation
tissuewasnotobserved,
andvaginal
shrinkage
didnotoccur.Thefinal resultwasrelated
directly
tothe motivation of thepatient
and heruseof the moldpostoperatively.
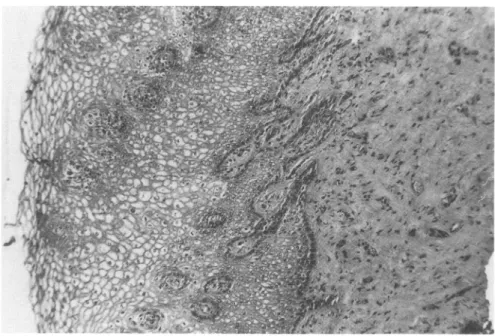
FIG. 3.
Vaginal biopsy
taken from thenewly
formedvaginal cavity
8 weeks after surgery.Maturevaginal epithelium.
Gomori's trichrome. x120.
DISCUSSION
Varioustreatmentshave been describedfor
vaginal agenesis. Frank1
'reported graduated
vaginal
dilatation,
butthis
technique
hasgiven good
results in less than 50% ofpatients. Williams'2
described the method ofaturned-in labial
flap.
Although
theprocedure
didnotrequire
anygraft,
nosatisfactory
resultswerereported.
Indeed,
thevaginal
axiswasoften illplaced,
and difficultiesatthe time of micturition andrepeated urinary
tractinfectionswereobserved.Creating
atunnel forcongenital
absence of thevagina
isastep
that iscommontoallsurgical procedures.
The use or nonuse ofagraft
could bediscussed,
and ifagraft
is tobeused,
which tissue isbest—skin,
intestine,
oramnion.Theuseof cecal or
sigmoid
bowelsegments
wasreported by Baldwin13
in 1904.Though
some authorsclaimed
good
results,
this method is amajor surgical procedure
withsignificant morbidity
andmortality.
Turner-Warwick and
Kirby14
havereported
successful reconstruction of thevagina
with the colocecum without serioussurgical
complication,
butprofuse
secretions,
persistent unpleasant
odor,
and ulcération of the mucosal surface could be themajor
side effects.Wharton15
devisedanoperation
basedonthe remarkableregenerative potential
ofgranulation
tissue in thevaginal
canal. Tokeep
the spacepatent,
acondom-covered moldwasused. Mclndoe andBannister1
modifiedWharton's
operation
by
the additionalstep
oftransplanting
asplit-thickness
skingraft
into thenewly
formedvaginal cavity
held inplace
by
avaginal
mold. Thegreat
variations in success rate,high
incidence ofpostoperative
infection,
necrosis of the skingraft,
andscarring,
however,
made it lessacceptable.
Moreover,
thepatient
suffers considerable discomfort from the donor skinsite,
which may remainvisible.Myocutaneous flaps
have been usedby
several authors. Thegracilis
myocutaneous
flap
has become verypopular
inrecentyears,l6~19butaseriousdisadvantage
is theprecarious vascularity
of theflaps.
In the seriesof McCrawet
al.20
of 22patients,
6 sufferedatotally
catastrophic
loss of theflap.
Therectusabdominisflap
is anotherpopular flap,
but thesingular complaint
about it is thelarge
abdominal donor-sitedefect,21
and theoperative
time islong.
The neurovascularpudendal thigh flap procedure
isafeasibleonethat alsocanbe usedreliably
to reconstructthevagina.
The results from all thetechniques
withflaps
describedpartial
flap
loss and necrosis inanunacceptable
failurerate.Moreover,
such dissections causedamajor
skin scarand could beindicated
only
forvaginal
reconstruction afterpelvectomy
forpelvic
cancer, whensubsequent
irradiation mustbe carriedout.Toovercomethese
difficulties,
amnion alone with the cleanmesenchymal
surfaceplaced
toward the host was usedby
several authors(Brindeau,2
Burger,3
Trelford etal.,6
andDhall9).
Dino etal.23
suggested
sterilizing
amniotic membranes. Trelfordetal.5'7
found that membranes stored at4°C in 0.5 N saline withantibioticsweresterileatthe end of 48 hours.
Inour
study,
amnioticmembranesweretakenimmediately
postpartum
(<
6hours).
Saline solution withantibioticswasneverused. Membraneswererinsed
only
in sterilephysiologic
solution(NaCl 0.9%).
Faulk et
al.24
have demonstratedmicroscopic
evidence ofnew vessel formation andsuggested
that anangiogenic
factor isproduced by
amnion.There isnoproblem
with immunerejection
because amnion doesnotexpress
histocompatibility antigens,
andAkleetal.25
foundnoevidenceoftissuerejection
when amnion wasimplanted subcutaneously
in volunteers. Tancer etal.8
Dhall,9
and Ashworth etal.10
havereported
successfulprocedures using
amnionas agraft
onvaginoplasties.
Removal of themoreantigenic
chorion hasbeen
suggested
tocontributetothesuccessfuluseof the amnion. In thepresent
study,
however,
the amnionwasnot
stripped
from the chorion. Our results show thevagina
tobe well formed and of normaldepth
andcaliber. There wasno
problem
of immunerejection.
Sexual intercoursewasreported
tobesatisfactory
in allcases.
Vaginal
smearsandvaginal
biopsy specimens
weretakenatfollow-up
visits.Vaginal epithelium
waspresent
by
8to 10 weeks.In
conclusion,
amniotic membranesreadily
available,
easily
stored,
andinexpensive
canbe used withoutsterilization as a
graft
forvaginal
reconstruction. The amniotic membranes adherefirmly,
protect
theunderlying
granulation,
and facilitateepithelialization. Hospitalization
isconsiderably
reduced,
andmajor
skin defectsoccurring
aftermyocutaneous
flap
reconstruction are avoided. Nopostoperative
dilatation isneededoncenormal sexual intercourse is resumed.
REFERENCES
1. MclndoeAH,Bannister JE. An
operation
for thecureofcongenital
absenceof thevagina.
JObstetGynaecol
BrEmp
1938;45:490.
2. Brindeau A. Création d'un
vagin
artificiel à l'aide des membranes ovulaires d'un oeufàterme.Gynecol
Obstet(Paris)
1934;29:385.3.
Burger
K. WeitereErfahrungen
über die kunstlicheScheidenbildung
mit Eihäuten. ZentralblGynaekol
1947:69:1153.4. TrelfordJD, Hanson FW, Anderson DG. Amniotic membrane as a
living surgical dressing
in humanpatients.
Oncology
1973;28:358.5. TrelfordJD,AndersonD,HansonF,MendelV. Amnioticmembrane usedforradical vulvectomies. Obstet
Gynecol
Observ 1973;12:1.6. Trelford JD, Hanson FW, Anderson DS. The
feasibility
ofmaking
an artificialvagina
atthe time of anterior exenteration.Oncology
1973;28:398.7. Trelford-Sauder M, Trelford JD, Matólo NM.
Replacement
of theperitoneum
with amnionfollowing pelvic
exenteration.Surg Gynecol
Obstet 1977:145:699.8. TancerML,KatzM,Veridiano NP.
Vaginal
epithelialization
with human amnion. ObstetGynecol
1979;54:345. 9. DhallK. Amniongraft
fortreatmentofcongenital
absence of thevagina.
BrJ ObstetGynaecol
1984;91:279. 10. Ashworth MF, Morton KE, Dewhurst J, Lilford RJ, Bates RG.Vaginoplasty
using
amnion. ObstetGynecol
1986;67:443.
11. Frank RT. The formation ofanartificial
vagina
withoutoperation.
Am JObstetGynecol
1938;35:1053.12. WilliamsEA.
Congenital
absence of thevagina—A simple operation
for its relief. J ObstetGynaecol
Br Commonw 1964;71:511.13. Baldwin JF. The formation ofanartificial
vagina by
intestinaltransplantation.
AnnSurg
1904;40:398.14. Turner-WarwickR,
Kirby
RS. The construction and reconstruction of thevagina
withthecolocecum.Surg Gynecol
Obstet 1990;170:132.
15. Wharton LR. A
simple
method ofconstructing
avagina.
AnnSurg
1938;107:842.16. HeathPM,WoodsJE, PodratzKC,ArnoldPG,IronsGB. Gracilismyocutaneous
vaginal
reconstruction.Mayo
Clin Proc1984;59:21.17.
Lagasse
LD,BermanML,Watting
WG,Ballon SC. Thegynecologic oncology patient:
Restoration offunction andprevention
ofdisability.
In: McGowan L, ed.Gynecologic oncology.
New York:Appleton-Century-Crofts,
1978:398.18.
Lacey
PM, Morrow CP.Myocutaneous
vaginal
reconstruction. In: Morrow CP, Smart GE, eds.Gynecologic
oncology.
Berlin:Springer-Verlag,
1986:255.19. Wheeless CR.
Vulvar-vaginal
reconstruction.In:Coppleson
M,ed.Gynecologic oncology:
Fundamentalprinciples
andclinical
practice. Edinburgh:
ChurchillLivingstone,
1981;2:933.20. McCrawJB,
Massey
FM,ShanklinKD,Horton CE.Vaginal
reconstruction withgracilis
myocutaneousflaps.
PlastReconstrSurg
1976;58:176.
21. Gordon RT, Thomas GD.
Vaginal
andpelvic
reconstruction withdistally
basedrectus abdominis myocutaneousflaps.
Plast ReconstrSurg
1988;71.22. Wee TK,
Joseph
VT. A newtechnique
ofvaginal
reconstructionusing
neurovascularpudendal-thigh flaps:
Apreliminary
report.Plast ReconstrSurg
1989;701.23. Diño BR, Eufemio GG, DeVilla MS. Human amnion: The establishment ofan amnion bank and its
practical
applications
insurgery. JPhilippine
Med Assoc 1966;42:357.24. FaulkWP,MatthewsR,StevensPJ, etal. Human amnionasan
adjunct
in woundhealing.
Lancet 1980;1:1156. 25. AkleCA,AdinolfiM,WelshKI,etal.Immunogenicity
of humanamnioticepithelial
cells aftertransplantation
intovolunteers.Lancet 1980;2:1003.
Address
reprint
requests
to:Professor
J. Donnez Headof Department
CatholicUniversity
of
LouvainAvenue