What are the topics of definition for multimorbidity recognized in polish general practice?
Texte intégral
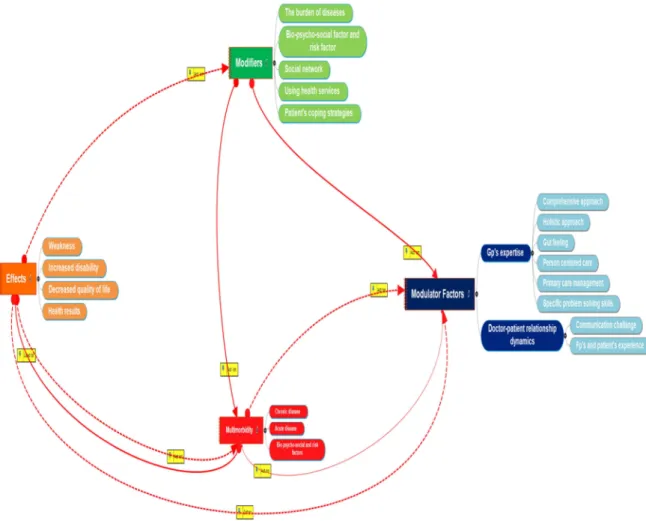
Figure

Documents relatifs
The control of the conditions to obtain the steel semisolid state represents a difficulty, but the results on the parts are quite satisfactory from a macro and microscopic point
Since the access point, AP, is considered as a normal contention- based mobile node, it has the same opportunity of sending packets (to all the download mobile nodes) as any of
A continued fraction expansion to the immittances defining viscothermal wave propagation in a cylindrical tube has been presented recently in this journal, intended as a starting
In section 10.2.2 of tender specification, it states that the Total Weighted Price of Profile is the “Sum of prices for the profile, with intra-muros prices (on Contracting
Researchers in the field of multimorbidity explored innovative research topics, themes, questions and appro- priate design formats in relation to the concept of Multi- morbidity for
The current study is based on a forward and backward translation of the original English defi - nition using a Delphi consensus procedure.. 15 The forward translation of MM
Disordered online behaviours, such as excessive video gaming, pornography viewing, buying, gam- bling, or streaming and social networks use ( Ioannidis et al., 2018 ) have
Before submitting a proposal, we wanted to check the approach with data from the previous campaign. In brief, we were looking for a fragment in the -4n channel in coincidence with
